

Virtual reality training improves operating room performance: results of a randomized, double-blinded study
- PMID: 12368674
- PMCID: PMC1422600
- DOI: 10.1097/00000658-200210000-00008
Virtual reality training improves operating room performance: results of a randomized, double-blinded study
Abstract
Objective: To demonstrate that virtual reality (VR) training transfers technical skills to the operating room (OR) environment.
Summary background data: The use of VR surgical simulation to train skills and reduce error risk in the OR has never been demonstrated in a prospective, randomized, blinded study.
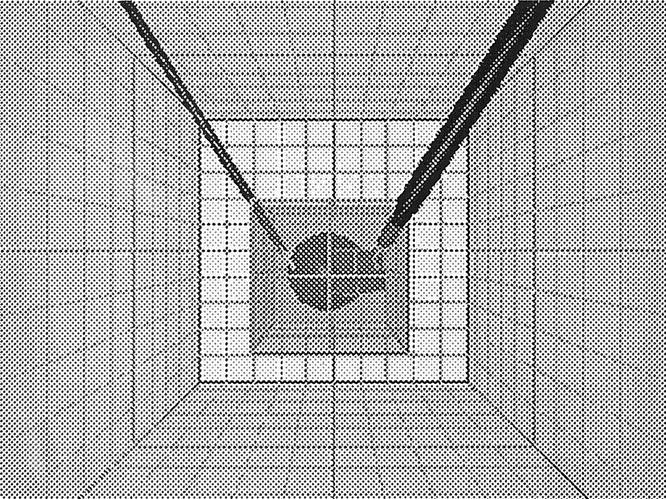
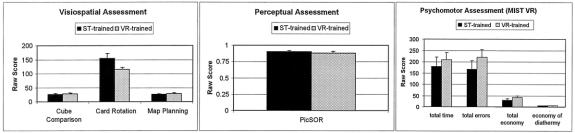
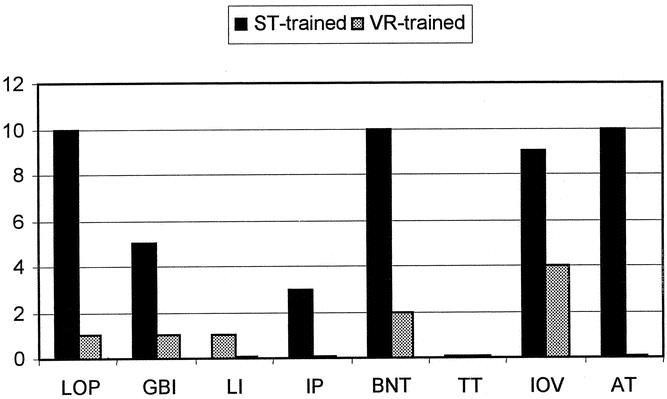
Methods: Sixteen surgical residents (PGY 1-4) had baseline psychomotor abilities assessed, then were randomized to either VR training (MIST VR simulator diathermy task) until expert criterion levels established by experienced laparoscopists were achieved (n = 8), or control non-VR-trained (n = 8). All subjects performed laparoscopic cholecystectomy with an attending surgeon blinded to training status. Videotapes of gallbladder dissection were reviewed independently by two investigators blinded to subject identity and training, and scored for eight predefined errors for each procedure minute (interrater reliability of error assessment r > 0.80).
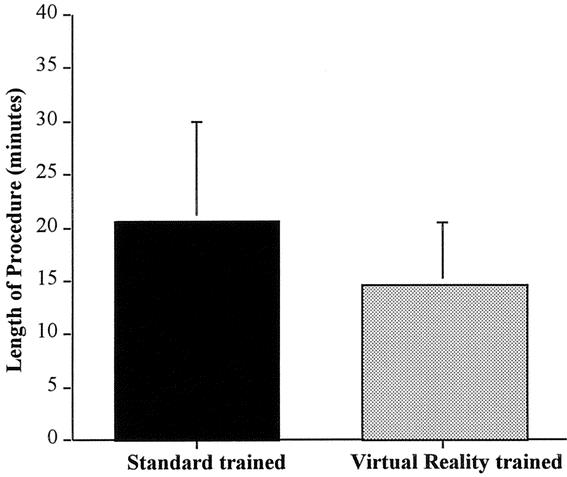
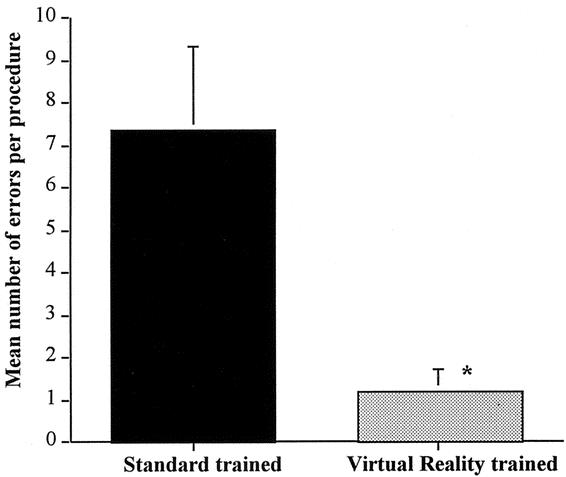
Results: No differences in baseline assessments were found between groups. Gallbladder dissection was 29% faster for VR-trained residents. Non-VR-trained residents were nine times more likely to transiently fail to make progress (P <.007, Mann-Whitney test) and five times more likely to injure the gallbladder or burn nontarget tissue (chi-square = 4.27, P <.04). Mean errors were six times less likely to occur in the VR-trained group (1.19 vs. 7.38 errors per case; P <.008, Mann-Whitney test).
Conclusions: The use of VR surgical simulation to reach specific target criteria significantly improved the OR performance of residents during laparoscopic cholecystectomy. This validation of transfer of training skills from VR to OR sets the stage for more sophisticated uses of VR in assessment, training, error reduction, and certification of surgeons.
Figures
References
-
- Deziel D, Milikan KW, Economou SG, et al. Complications of laparoscopic cholecystectomy: A national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg 1993; 165: 9–14. - PubMed
-
- The Southern Surgeons Club. The learning curve for laparoscopic cholecystectomy. Am J Surg 1995; 170: 55–59. - PubMed
-
- Senate of Surgery. Response to the General Medical Council Determination on the Bristol Case. London: Senate Paper 5, The Senate of Surgery of Great Britain and Ireland, 1998.
-
- Kohn LT, Corrigan JM, Donaldson M. To Err is Human: Building a Safer Health System. Washington, DC: Institute of Medicine, 1999. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
