

Long-term results of local excision for rectal cancer
- PMID: 12368681
- PMCID: PMC1422607
- DOI: 10.1097/00000658-200210000-00015
Long-term results of local excision for rectal cancer
Abstract
Objective: To review the authors' experience with local excision of early rectal cancers to assess the effectiveness of initial treatment and of salvage surgery.
Summary background data: Local excision for rectal cancer is appealing for its low morbidity and excellent functional results. However, its use is limited by inability to assess regional lymph nodes and uncertainty of oncologic outcome.
Methods: Patients with T1 and T2 adenocarcinomas of the rectum treated by local excision as definitive surgery between 1969 to 1996 at the authors' institution were reviewed. Pathology slides were reviewed. Among 125 assessable patients, 74 were T1 and 51 were T2. Thirty-one patients (25%) were selected to receive adjuvant radiation therapy. Fifteen of these 31 patients received adjuvant radiation in combination with 5-fluorouracil chemotherapy. Median follow-up was 6.7 years. One hundred fifteen patients (92%) were followed until death or for greater than 5 years, and 69 patients (55%) were followed until death or for greater than 10 years. Recurrence was recorded as local, distant, and overall. Survival was disease-specific.
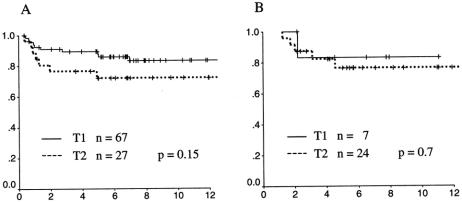
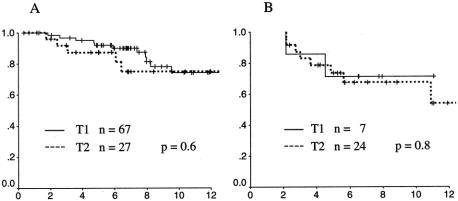
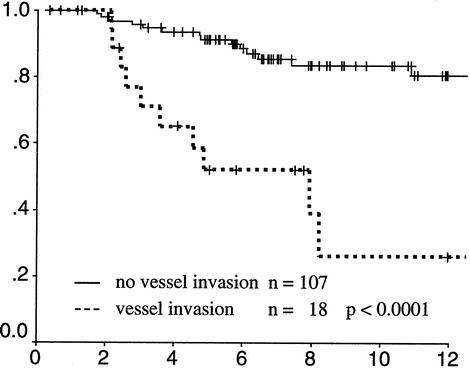
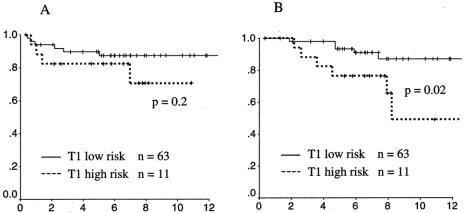
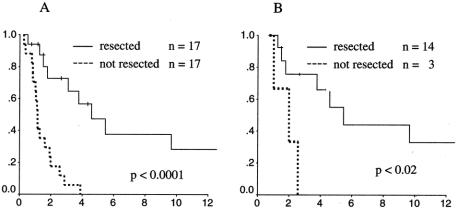
Results: Ten-year local recurrence and survival rates were 17% and 74% for T1 rectal cancers and 26% and 72% for T2 cancers. Median time to relapse was 1.4 years (range 0.4-7.0) for local recurrence and 2.5 years (0.8-7.5) for distant recurrence. In patients receiving radiotherapy, local recurrence was delayed (median 2.1 years vs. 1.1 years), but overall rates of local and overall recurrence and survival rates were similar to patients not receiving radiotherapy. Among 26 cancer deaths, 8 (28%) occurred more than 5 years after local excision. On multivariate analysis, no clinical or pathologic features were predictive of local recurrence. Intratumoral vascular invasion was the only significant predictor of survival. Among 34 patients who developed tumor recurrence, the pattern of first clinical recurrence was predominantly local: 50% local only, 18% local and distant, and 32% distant only. Among the 17 patients with isolated local recurrence, 14 underwent salvage resection. Actuarial survival among these surgically salvaged patients was 30% at 6 years after salvage. CONCLUSIONS The long-term risk of recurrence after local excision of T1 and T2 rectal cancers is substantial. Two thirds of patients with tumor recurrence have local failure, implicating inadequate resection in treatment failure. In this study, neither adjuvant radiotherapy nor salvage surgery was reliable in preventing or controlling local recurrence. The postoperative interval to cancer death is as long as 10 years, raising concern that cancer mortality may be higher than is generally appreciated. Additional treatment strategies are needed to improve the outcome of local excision.
Figures
References
-
- Enker WE, Havenga K, Polyak T, et al. Abdominoperineal resection via total mesorectal excision and autonomic nerve preservation for low rectal cancer. World J Surg 1997; 21: 715–720. - PubMed
-
- Rothenberger DA, Wong WD. Abdominoperineal resection for adenocarcinoma of the low rectum. World J Surg 1992; 16: 478–485. - PubMed
-
- Averbach AM, Chang D, Koslowe P, et al. Anastomotic leak after double-stapled low colorectal resection. Dis Colon Rectum 1996; 39: 780–787. - PubMed
-
- Williamson ME, Lewis WG, Finan PJ, et al. Recovery of physiologic and clinical function after low anterior resection of the rectum for carcinoma: myth or reality? Dis Colon Rectum 1995; 38: 411–418. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
