

First-line treatment for advanced ovarian cancer: paclitaxel, platinum and the evidence
- PMID: 12373593
- PMCID: PMC2376171
- DOI: 10.1038/sj.bjc.6600567
First-line treatment for advanced ovarian cancer: paclitaxel, platinum and the evidence
Abstract
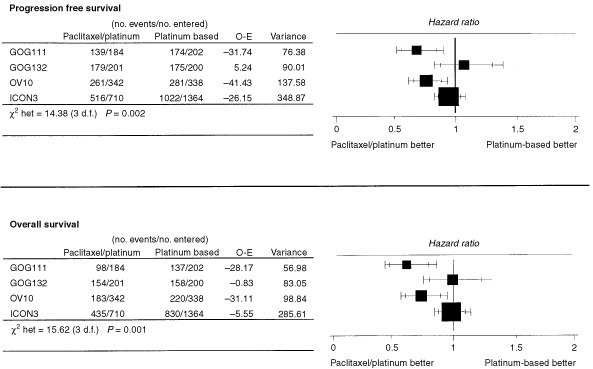
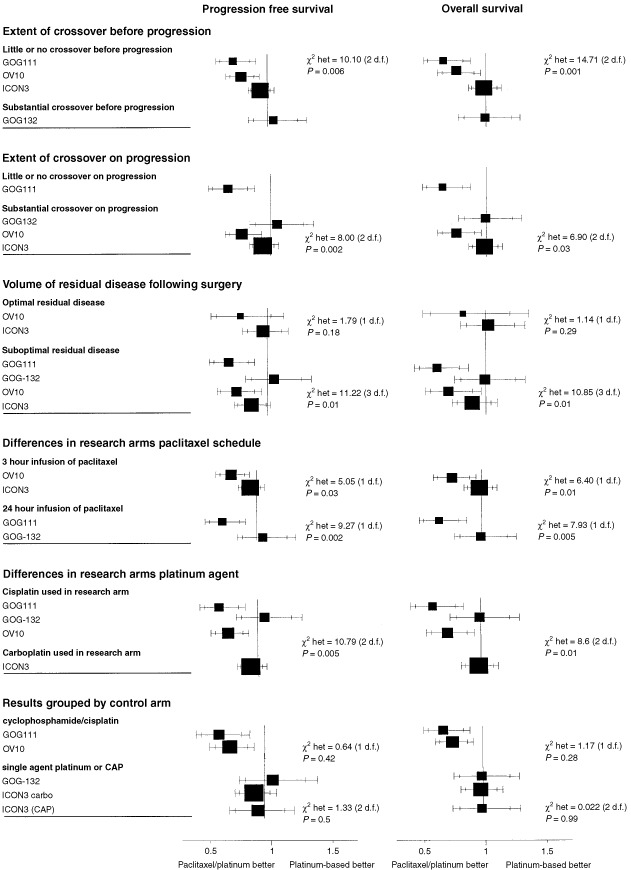
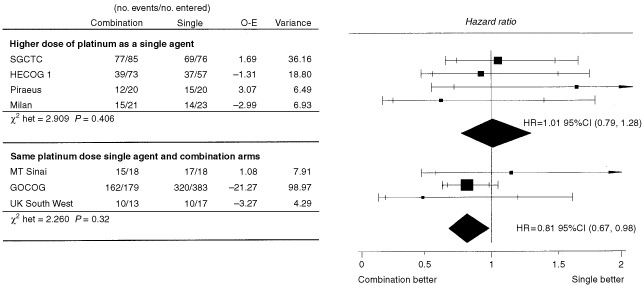
Four large randomised trials of paclitaxel in combination with platinum against a platinum-based control treatment have now been published in full, representing around 88% (3588 out of 4057) of patients randomised into the eight known trials of this question. There is substantial heterogeneity in the results of these four trials. Four main explanations for this heterogeneity have been proposed: differences in the extent and timing of 'crossover' to taxanes in the control groups; differences in the types of patient included; differences in the effectiveness of the research regimens used; differences in the effectiveness of the control regimens used. In this study we examine whether any of these explanations is consistent with the pattern of results seen in these trials. Each explanation suggests that a particular characteristic of each trial was responsible for the results observed. For each explanation the trials were split into groups according to that characteristic, in order to partition the total heterogeneity into that seen 'within' and 'between' groups of trials. If a particular explanation was consistent with the pattern of results, we would expect to see relatively little heterogeneity within each group of trial results viewed in this way, with most of the heterogeneity being between groups which are dissimilar with respect to the key characteristic. Heterogeneity 'within' and 'between' groups was formally compared using the F-ratio. If any explanation appeared to be consistent with the results of the trials, it was considered whether the explanation was also consistent with other evidence available about these regimens. Only one explanation appeared to be consistent with the pattern of results seen in these trials, and that was differences in effectiveness of the control arms used in these trials. This suggests that the very positive results in favour of paclitaxel/cisplatin seen in two of the trials may have been due to the use of a suboptimal control arm. There is no direct evidence about the relative effectiveness of the control arms used in these trials, but indirect evidence is consistent with the conclusion that the cyclophosphamide/cisplatin regimen used in two of the trials may be less effective than the control regimens used in the other trials. Specific concerns about the choice of a cyclophosphamide/cisplatin control arm in the first of these trials to report were raised before the results of the other trials were known, i.e. before any heterogeneity had been observed. Further investigation of this question would be useful. In the meantime, given all of the randomised evidence on the efficacy and toxicity associated with the regimens used in these trials, we conclude that single agent carboplatin is a safe and effective first-line treatment for women with advanced ovarian cancer.
Copyright 2002 Cancer Research UK
Figures
References
-
- AdamsMA'HernRPCalvertAHCarmichaelJClarkPIColemanREEarlHMGallagherCJGanesanTSGoreMEGrahamJDHarperPGJaysonGCKayeSBLedermannJAOsborneRJPerrenTJPooleCJRadfordJARustinGJSlevinMLSmythJFThomasHWilkinsonPM1998Chemotherapy for ovarian cancer – a consensus statement on standard practice Br J Cancer 7814041406 - PMC - PubMed
-
- AdamsMKerbyIJRockerIEvansAJohansenKFranksCR1989A comparison of toxicity and efficacy of cisplatin and carboplatin in advanced ovarian cancer Acta Oncol 285760 - PubMed
-
- AthanassiouAVarthalitisJTsavarisNDimitriadisMMoutzouridisG1997Superiority of carboplatin monochemotherapy over carboplatin-based polychemotherapy in ovarian cancer Eur J Gynaecol Oncol 18420425 - PubMed
-
- BolisGFavalliGDaneseSZanaboniFMangiliGScarabelliCTateoSValsecchiMGScarfoneGRichiardiGFrigerioLMelpignanoMVillaAParazziniF1997Weekly cisplatin given for 2 months versus cisplatin plus cyclophosphamide given for 5 months after cytoreductive surgery for advanced ovarian cancer J Clin Oncol 1519381944 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
