

Prognosis of malignant intraductal papillary mucinous tumours of the pancreas after surgical resection. Comparison with pancreatic ductal adenocarcinoma
- PMID: 12377813
- PMCID: PMC1773420
- DOI: 10.1136/gut.51.5.717
Prognosis of malignant intraductal papillary mucinous tumours of the pancreas after surgical resection. Comparison with pancreatic ductal adenocarcinoma
Abstract
Background: Although the prognosis in malignant resectable intraductal papillary mucinous tumours of the pancreas (IPMT) is often considered more favourable than for ordinary pancreatic ductal adenocarcinoma, the long term outcome remains ill defined.
Aims: To assess prognostic factors in patients with malignant IPMT after surgical resection, and to compare long term survival rates with those of patients surgically treated for ductal adenocarcinoma.
Methods: Seventy three patients underwent surgery for malignant IPMT in four French centres. Clinical, biochemical, and pathological features and follow up after resection were recorded. Patients with invasive malignant IPMT were matched with patients with pancreatic ductal adenocarcinoma, according to age and TNM stages; survival rates after resection were compared.
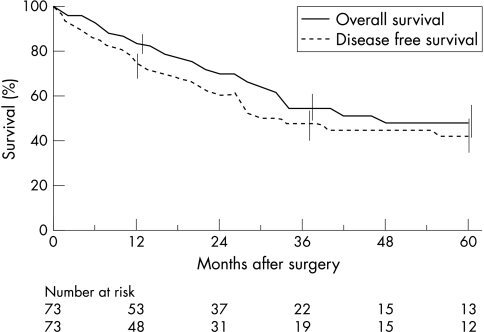
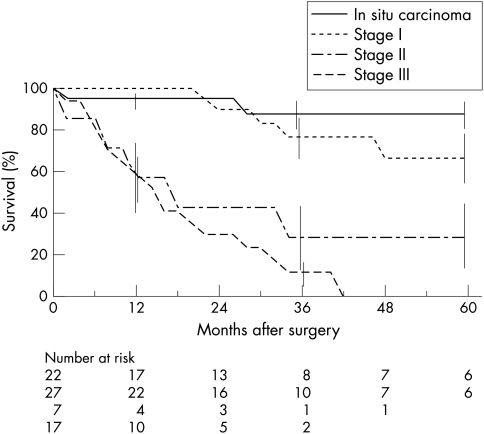
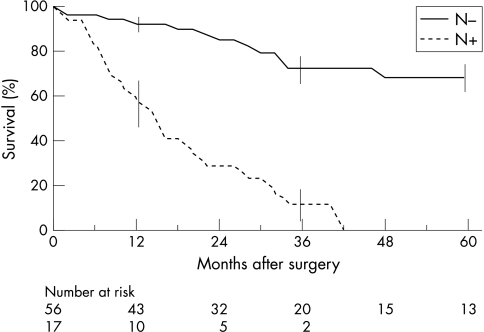
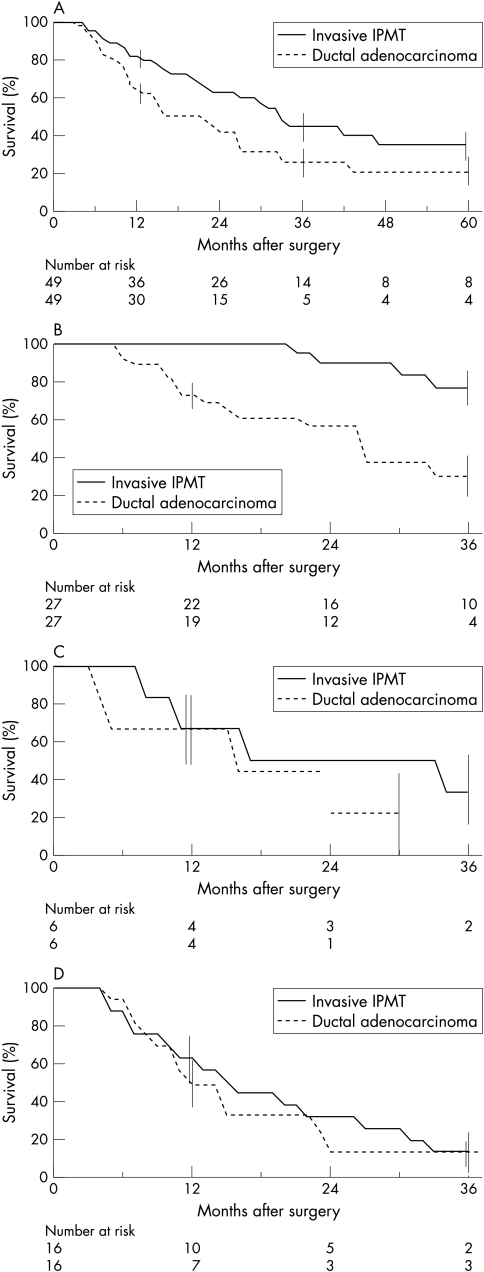
Results: Surgical treatment for IPMT were pancreaticoduodenectomy (n=46), distal (n=14), total (n=11), or segmentary (n=2) pancreatectomy. The operative mortality rate was 4%. IPMT corresponded to in situ (n=22) or invasive carcinoma (n=51). In the latter group, 17 had lymph node metastases. Overall median survival was 47 months. Five year survival rates in patients with in situ and invasive carcinoma were 88% and 36%, respectively. On univariate analysis, abdominal pain, preoperative high serum carbohydrate antigen 19.9 concentrations, caudal localisation, invasive carcinoma, lymph node metastases, peripancreatic extension, and malignant relapse were associated with a fatal outcome. Using multivariate analysis, lymph node metastases were the only prognostic factor (OR 7.5; 95% CI: 3.4 to 16.4). Overall five year survival rate was higher in patients with malignant invasive IPMT compared with those with pancreatic ductal carcinoma (36 v 21%, p=0.03), but was similar in the subset of stage II/III tumours.
Conclusions: The prognosis of patients with resected in situ/invasive stage I malignant IPMT is excellent. In contrast, prognosis of locally advanced forms is as poor as in patients with pancreatic ductal adenocarcinoma.
Figures
References
-
- Loftus EV Jr, Olivares-Pakzad BA, Batts KP, et al. Intraductal papillary-mucinous tumors of the pancreas: clinicopathologic features, outcome, and nomenclature. Gastroenterology 1996;110:1909–18. - PubMed
-
- Itai Y, Ohhashi K, Nagai H, et al. “ Ductectatic “ mucinous cystadenoma and cystadenocarcinoma of the pancreas. Radiology 1986;161:697–700. - PubMed
-
- Klöppel G, Solcia E, Longnecker DS, et al. Histological typing of tumours of the exocrine pancreas. 2nd edn. In: World Health Organisation. International histological classification of tumours. Berlin: Springer-Verlag, 1996.
-
- Barbe L, Ponsot P, Vilgrain V, et al. Tumeurs intra-canalaires papillaires mucineuses pancréatiques. Aspects cliniques et morphologiques chez 30 malades. Gastroenterol Clin Biol 1997;21:278–86. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical