

Clinical and immune impact of Mycobacterium bovis BCG vaccination scarring
- PMID: 12379697
- PMCID: PMC130324
- DOI: 10.1128/IAI.70.11.6188-6195.2002
Clinical and immune impact of Mycobacterium bovis BCG vaccination scarring
Abstract
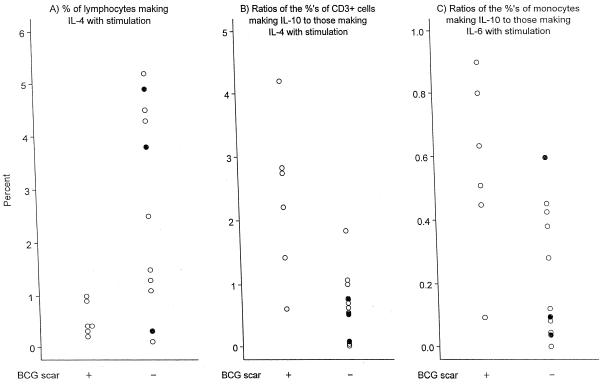
The World Health Organization recommends Mycobacterium bovis BCG vaccination in areas of high tuberculosis prevalence. BCG's clinical and immune effects, not necessarily Mycobacterium tuberculosis specific, are unclear. BCG vaccine scarring often is used as a surrogate marker of vaccination or of effective vaccination. We evaluated BCG scarring status in relation to clinical findings and outcome in 700 hospitalized Malawians, of whom 32 had M. tuberculosis bloodstream infections (BSI) (10 of whom had cellular immune studies done) and of whom 48 were infants <6 months old and therefore recently vaccinated (19 of whom had immune studies). In the patients >/=6 months old, scarring was not related to the presence of pulmonary symptoms (35 versus 30%), chronic cough or fever, mortality, or M. tuberculosis BSI. In M. tuberculosis BSI patients, scarring was unrelated to mortality, vital signs, or clinical symptoms but those with scarring had higher proportions of memory and activated T cells and more type 2-skewed cytokine profiles. Infants with either BCG scarring (n = 10) or BCG lesional inflammation (n = 5) had no symptoms of sepsis, but 18 of 33 infants without BCG vaccination lesions did. Those with BCG lesions had localized infections more often than did those without BCG lesions. These infants also had lower median percentages of lymphocytes spontaneously making interleukin-4 (IL-4) or tumor necrosis factor alpha (TNF-alpha) and lower ratios of T cells spontaneously making IL-4 to T cells making IL-6. Thus, we found that, in older patients, BCG vaccine scarring was not associated with M. tuberculosis-specific or nonspecific clinical protection. Those with M. tuberculosis BSI and scarring had immune findings suggesting previous M. tuberculosis antigen exposure and induction of a type 2 cytokine pattern with acute reexposure. It is unlikely that this type 2 pattern would be protective against mycobacteria, which require a type 1 response for effective containment. In infants <6 months old, recent BCG vaccination was associated with a non-M. tuberculosis-specific, anti-inflammatory cytokine profile. That the vaccinated infants had a greater frequency of localized infections and lesser frequency of sepsis symptoms suggests that this postvaccination cytokine pattern may provide some non-M. tuberculosis-specific clinical benefits.
Figures
References
-
- Archibald, L. K., L. C. McDonald, R. M. Addison, C. M. McKnight, T. C. Byrne, O. Nwanyanwu, P. Kazembe, H. Dobbie, L. B. Reller, and W. R. Jarvis. 2000. A comparison of Myco-F-Lytic and Lysis-Centrifugation isolator systems for detection of bacteremia, mycobacteremia, and fungemia in febrile hospitalized patients, Lilongwe, Malawi. J. Clin. Microbiol. 38:2994-2997. - PMC - PubMed
-
- Awasthi, S., and S. Moin. 1999. Effectiveness of BCG vaccination against tuberculous meningitis. Indian Pediatr. 36:455-460. - PubMed
-
- Bloom, B. R., and P. E. M. Fine. 1994. The BCG experience: implications for future vaccines against tuberculosis, p. 531-537. In R. B. Bloom (ed.), Tuberculosis: pathogenesis, protection, and control. American Society for Microbiology, Washington, D.C.
-
- Chhatwal, J., M. Verma, N. Thaper, and R. Aneja. 1994. Waning of post vaccinal allergy after neonatal BCG vaccination. Indian Pediatr. 31:1529-1533. - PubMed
-
- Colditz, G. A., C. S. Berkey, F. Mosteller, T. F. Brewer, M. E. Wilson, E. Burdick, and H. V. Fineberg. 1995. The efficacy of bacille Calmette-Guerin vaccination of newborns and infants in the prevention of tuberculosis: meta-analysis of the published literature. Pediatrics 96:29-35. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
