

Conventional treatments for ankylosing spondylitis
- PMID: 12381510
- PMCID: PMC1766726
- DOI: 10.1136/ard.61.suppl_3.iii40
Conventional treatments for ankylosing spondylitis
Abstract
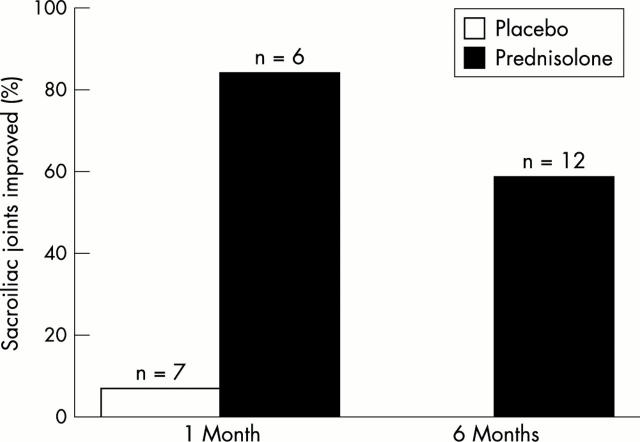
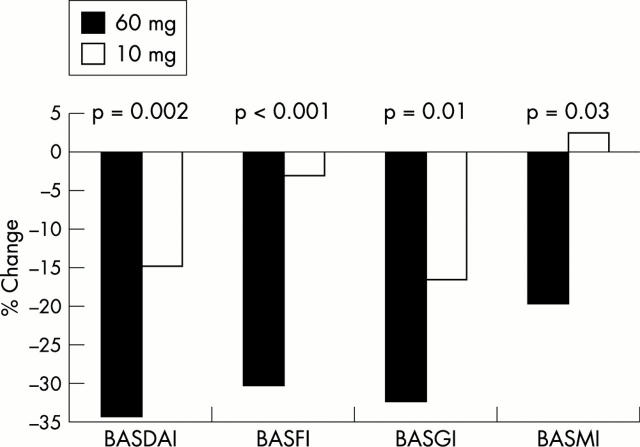
Management of ankylosing spondylitis (AS) is challenged by the progressive nature of the disease. To date, no intervention is available that alters the underlying mechanism of inflammation in AS. Currently available conventional treatments are palliative at best, and often fail to control symptoms in the long term. Current drug treatment may perhaps induce a spurious state of "disease remission," which is merely a low level of disease activity. Non-steroidal anti-inflammatory drugs are first line treatment, but over time, the disease often becomes refractory to these agents. Disease modifying antirheumatic drugs are second line treatment and may offer some clinical benefit. However, conclusive evidence of the efficacy of these drugs from large placebo controlled trials is lacking. Additionally, these drugs can cause treatment-limiting adverse effects. Intra-articular corticosteroid injection guided by arthrography, computed tomography, or magnetic resonance imaging is an effective means of reducing inflammatory back pain, but controlled studies are lacking. A controlled study has confirmed moderate but significant efficacy of intravenous bisphosphonate (pamidronate) treatment in patients with AS; further evaluation of bisphosphonate treatment is warranted. Physical therapy and exercise are necessary adjuncts to pharmacotherapy; however, the paucity of controlled data makes it difficult to identify the best way to administer these interventions. Surgical intervention may be required to support severe structural damage. Thus, for patients with AS, the future of successful treatment lies in the development of pharmacological agents capable of both altering the disease course through intervention at sites of disease pathogenesis, and controlling symptoms.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
