

Non-invasive coronary angiography with multislice spiral computed tomography: impact of heart rate
- PMID: 12381635
- PMCID: PMC1767415
- DOI: 10.1136/heart.88.5.470
Non-invasive coronary angiography with multislice spiral computed tomography: impact of heart rate
Abstract
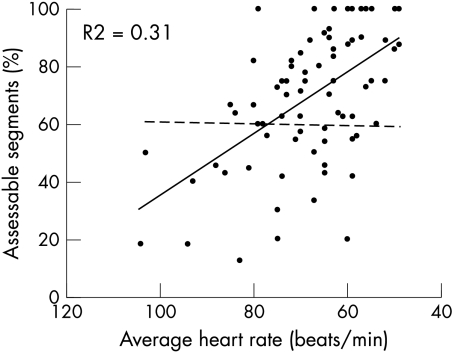
Objective: To evaluate the impact of heart rate on the diagnostic accuracy of coronary angiography by multislice spiral computed tomography (MSCT).
Design: Prospective observational study.
Patients: 78 patients who underwent both conventional and MSCT coronary angiography for suspicion of de novo coronary artery disease (n=53) or recurrent coronary artery disease after percutaneous intervention (n=25).
Setting: Tertiary referral centre.
Methods: Intravenously contrast enhanced MSCT coronary angiography was done during a single breath hold, and ECG synchronised images were reconstructed retrospectively. All coronary segments of > or = 2.0 mm without stents were evaluated by two investigators and compared with quantitative coronary angiography. Patients were classified according to the average heart rate (mean (SD)) into three equally sized groups: group 1, 55.8 (4.1) beats/min; group 2, 66.6 (2.8) beats/min; group 3, 81.7 (8.8) beats/min.
Results: Image quality was sufficient for analysis in 78% of the coronary segments in patients in group 1, 73% in group 2, and 54% in group 3 (p < 0.01). The sensitivity and specificity for detecting significant stenoses (> or = 50% lumen reduction) in these assessable segments were: 97% (95% confidence interval (CI) 84% to 100%) and 96% in group 1; 74% (52% to 89%) and 94% in group 2; and 67% (33% to 90%) and 94% in group 3 (p < 0.05). Accounting for all segments of > or = 2.0 mm, including lesions in non-assessable segments as false negatives, the sensitivity decreased to 82% (28/34 lesions, 95% CI 69% to 91%), 61% (14/23 lesions, 42% to 77%), and 32% (6/19 lesions, 15% to 50%), respectively (p < 0.01).
Conclusions: MSCT allows reliable coronary angiography in patients with low heart rates.
Figures




References
-
- Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography with multi-slice computed tomography. Lancet 2001;357:599–603. - PubMed
-
- Achenbach S, Giesler T, Ropers D, et al. Detection of coronary artery stenoses by contrast-enhanced, retrospectively electrocardiographically-gated, multislice spiral computed tomography. Circulation 2001;103:2535–8. - PubMed
-
- Knez A, Becker C, Leber A, et al. Non-invasive angiography with multi-detector helical computed tomography for evaluation of coronary artery disease [abstract]. J Am Coll Cardiol 2000;101(suppl A):463.
-
- Schroeder S, Kopp AF, Baumbach A, et al. Noninvasive detection and evaluation of atherosclerotic coronary plaques with multislice computed tomography. J Am Coll Cardiol 2001;37:1430–5. - PubMed
-
- Ohnesorge B, Flohr T, Becker C, et al. Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology 2000;217:564–71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical