

Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial
- PMID: 12389836
- PMCID: PMC126506
Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial
Abstract
Background: Delirium is common and often goes undetected in older patients admitted to medical services. It is associated with poor outcomes. We conducted a randomized clinical trial to determine whether systematic detection and multidisciplinary care of delirium in older patients admitted to a general medical service could reduce time to improvement in cognitive status.
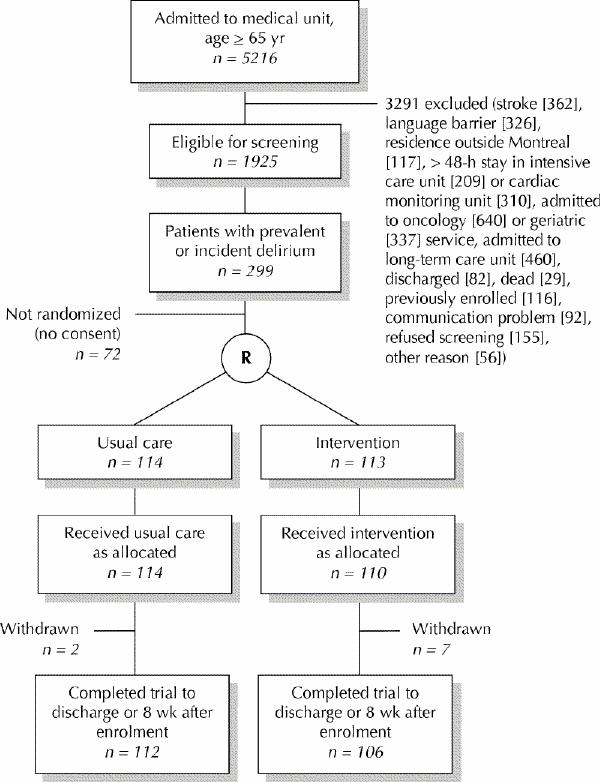
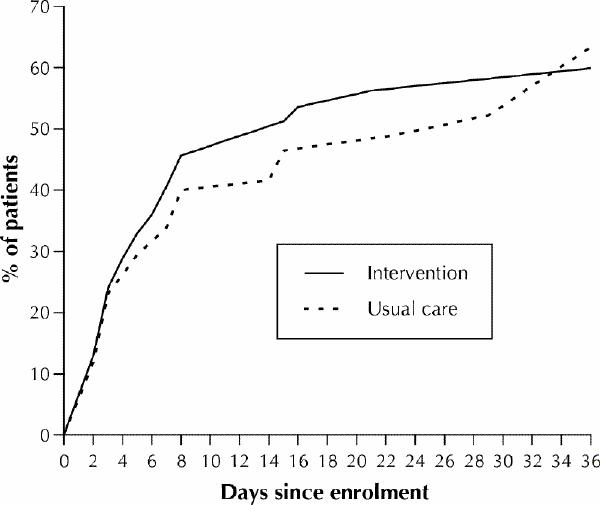
Methods: Consecutive patients aged 65 or more who were newly admitted to 5 general medical units between Mar. 15, 1996, and Jan. 31, 1999, were screened with the Confusion Assessment Method within 24 hours after admission to detect prevalent delirium and rescreened within a week to detect incident cases. Patients with delirium were randomly allocated to receive the intervention or usual care. Subjects in the intervention group were seen by a geriatric specialist consultant and followed in hospital for up to 8 weeks by an intervention nurse who liaised with the consultant, attending physicians, family and the primary care nurses. Subjects in the usual care group received standard hospital services but could consult geriatric specialists as needed. A research assistant, blinded as to treatment allocation, administered within 24 hours after enrolment the MiniMental Status Exam (MMSE), Delirium Index (measuring the severity of the delirium) and Barthel Index (measuring independence of personal care). Improvement was defined as an increase in the MMSE score of 2 or more points, with no decrease below baseline plus 2 points, or no decrease below a baseline MMSE score of 27. A short form of the Informant Questionnaire on Cognitive Decline in the Elderly was completed to identify patients with possible dementia. Subjects were assessed 3 times during the first week and weekly thereafter for up to 8 weeks in hospital or until discharge. Data on clinical severity of illness, length of stay and living arrangements after discharge were also collected. The primary outcome measure was time to improvement in MMSE score.
Results: Of the 1925 patients who met the inclusion criteria and were screened, 227 had prevalent or incident delirium and consented to participate (113 in intervention group and 114 in usual care group). There were no clinically significant differences between the intervention and usual care groups except for sex (female 58.4% v. 50.0%) and marital status (married 34.8% v. 41.2%). Overall, 48% of the patients in the intervention group and 45% of those in the usual care group met the predetermined criteria for improvement. The Cox proportional hazards ratio (HR) for a shorter time to improvement with the intervention versus usual care, adjusted for age, sex and marital status, was 1.10 (95% confidence interval [CI] 0.74-1.63). There were no significant differences within 8 weeks after enrolment between the 2 groups in time to and rate of improvement of the Delirium Index, the Barthel Index, length of stay, rate of discharge to the community, living arrangements after discharge or survival. Outcomes between the 2 groups did not differ statistically significantly for patients without dementia (HR 1.54, 95% CI 0.80-2.97), for those who had less co-morbidity (HR 1.36, 95% CI 0.75-2.46) or for those with prevalent delirium (HR 1.15, 95% CI 0.48-2.79).
Interpretation: Systematic detection and multidisciplinary care of delirium does not appear to be more beneficial than usual care for older patients admitted to medical services.
Figures
Comment in
-
Out of the furrow and into the fire: where do we go with delirium?CMAJ. 2002 Oct 1;167(7):763-4. CMAJ. 2002. PMID: 12389838 Free PMC article. No abstract available.
-
Studying delirium.CMAJ. 2003 Mar 4;168(5):541; author reply 541-2. CMAJ. 2003. PMID: 12615740 Free PMC article. No abstract available.
References
-
- Lipowski Z. Delirium: acute confusional states. New York: Oxford University Press; 1990.
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3rd rev ed. Washington: The Association; 1987. p. 103.
-
- Thomas RI, Cameron DJ, Fahs MC. A prospective study of delirium and prolonged hospital stay: exploratory study. Arch Gen Psychiatry 1988;45: 937-40. - PubMed
-
- Rockwood K. The occurrence and duration of symptoms in elderly patients with delirium. J Gerontol 1993;48(4):M162-6. - PubMed
-
- Chisholm S, Deniston L, Igrisan R, Barbus A. Prevalence of confusion in elderly hospitalized patients. J Gerontol Nurs 1982;8(2):87-96. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous