

Long-term effects of a collaborative care intervention in persistently depressed primary care patients
- PMID: 12390549
- PMCID: PMC1495114
- DOI: 10.1046/j.1525-1497.2002.11051.x
Long-term effects of a collaborative care intervention in persistently depressed primary care patients
Abstract
Objective: A previous study described the effect of a collaborative care intervention on improving adherence to antidepressant medications and depressive and functional outcomes of patients with persistent depressive symptoms 8 weeks after the primary care physician initiated treatment. This paper examined the 28-month effect of this intervention on adherence, depressive symptoms, functioning, and health care costs.
Design: Randomized trial of stepped collaborative care intervention versus usual care.
Setting: HMO in Seattle, Wash.
Patients: Patients with major depression were stratified into severe and moderate depression groups prior to randomization.
Interventions: A multifaceted intervention targeting patient, physician, and process of care, using collaborative management by a psychiatrist and a primary care physician.
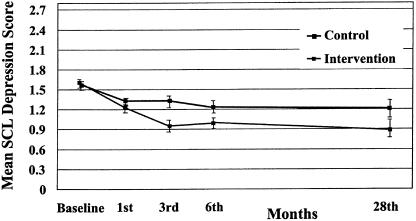
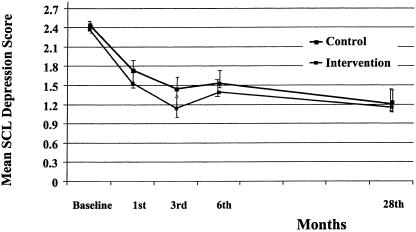
Measures and main results: The collaborative care intervention was associated with continued improvement in depressive symptoms at 28 months in patients in the moderate-severity group (F1,87 = 8.65; P =.004), but not in patients in the high-severity group (F1,51 = 0.02; P =.88) Improvements in the intervention group in antidepressant adherence were found to occur for the first 6 months (chi2(1) = 8.23; P <.01) and second 6-month period (chi2(1) = 5.98; P <.05) after randomization in the high-severity group and for 6 months after randomization in the moderate-severity group(chi2(1) = 6.10; P <.05). There were no significant differences in total ambulatory costs between intervention and control patients over the 28-month period (F1,180 = 0.77; P =.40).
Conclusions: A collaborative care intervention was associated with sustained improvement in depressive outcomes without additional health care costs in approximately two thirds of primary care patients with persistent depressive symptoms.
Figures
Comment in
-
Life after primary care depression quality improvement intervention.J Gen Intern Med. 2002 Oct;17(10):811. doi: 10.1046/j.1525-1497.2002.20804.x. J Gen Intern Med. 2002. PMID: 12390558 Free PMC article. No abstract available.
References
-
- Katon W, Von Korff M, Lin E, et al. Collaborative management to achieve treatment guidelines: impact on depression in primary care. JAMA. 1995;273:1026–31. - PubMed
-
- Katon W, Robinson P, Von Korff M, et al. A multifaceted intervention to improve treatment of depression in primary care. Arch Gen Psychiatry. 1996;53:924–32. - PubMed
-
- Simon G, Von Korff M, Heiligenstein J, et al. Fluoxetine versus tricyclic antidepressants: a randomized trial of effectiveness and cost in primary care. JAMA. 1996;275:1897–905. - PubMed
-
- Wells K, Sherbourne C, Schoenbaum M, et al. Impact of dissemination quality improvement programs for depression in managed primary care: a randomized controlled trial. JAMA. 2000;283:212–20. - PubMed
-
- Hunkeler E, Meresman J, Hargreaves W, et al. Efficacy of nurse telehealth care and peer support in augmenting treatment of depression in primary care. Arch Fam Med. 2000;9:700–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical