

Glycosaminoglycans are a potential cause of rheumatoid arthritis
- PMID: 12391302
- PMCID: PMC137889
- DOI: 10.1073/pnas.222536599
Glycosaminoglycans are a potential cause of rheumatoid arthritis
Abstract
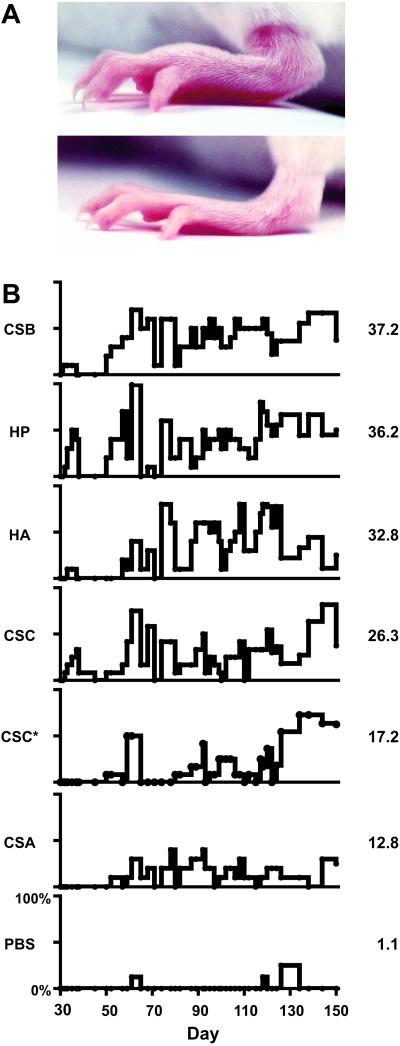
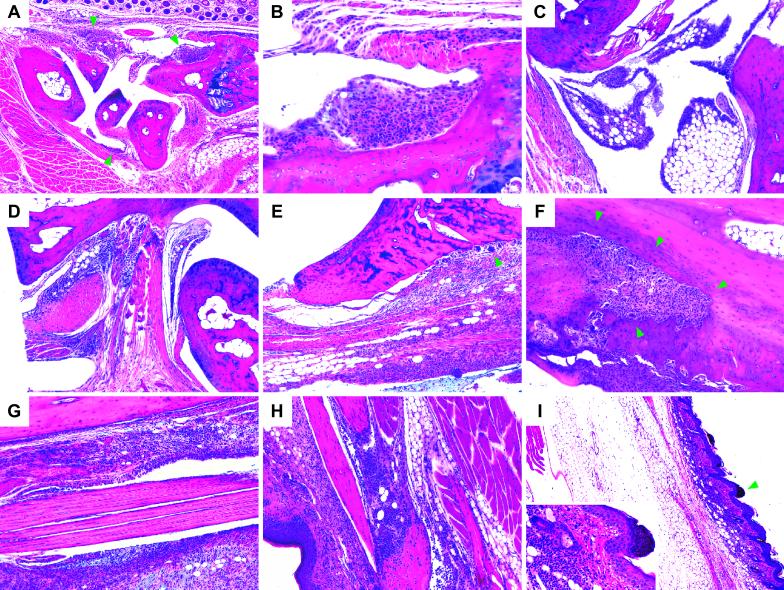
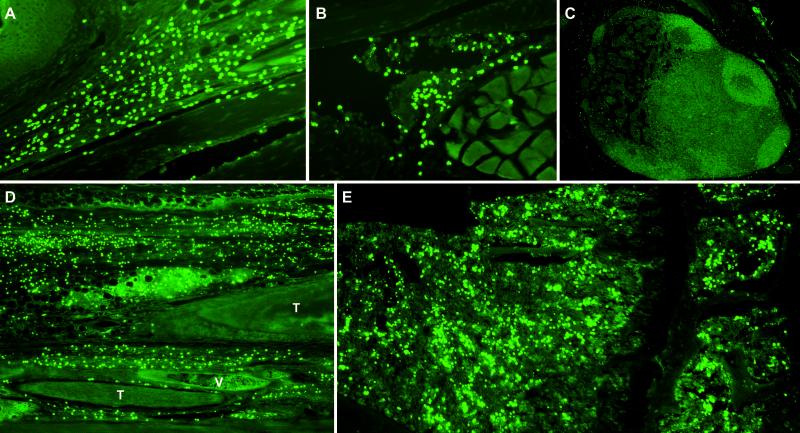
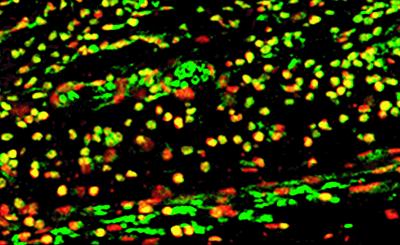
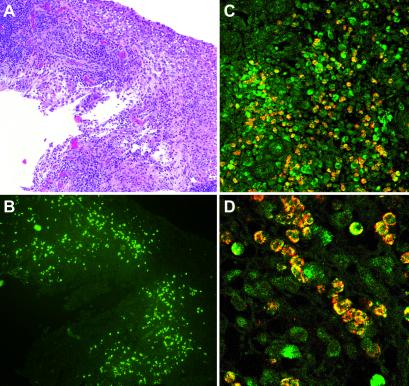
Rheumatoid arthritis (RA) is a chronic, systemic, and inflammatory disease of connective tissue with unknown etiology. We investigated whether aberrant immune responses to glycosaminoglycans (GAGs), a major component of joint cartilage, joint fluid, and other soft connective tissue, causes this disease. Here we show that injection of GAGs such as hyaluronic acid, heparin, and chondroitin sulfates A, B, and C induce arthritis, tendosynovitis, dermatitis, and other pathological conditions in mice. We developed a technique by staining tissue specimens with fluorochrome- or biotin-labeled GAGs to visualize the direct binding between cells and GAGs. We discovered that inflammatory infiltrates from the affected tissue are dominated by a distinct phenotype of GAG-binding cells, a significant portion of which are CD4(+) T cells. GAG-binding cells seem to be expanded in bone marrow of GAG-immunized mice. Furthermore, we identified GAG-binding cells in inflamed synovial tissue of human patients with RA. Our findings suggest that carbohydrate self-antigenic GAGs provoke autoimmune dysfunctions that involve the expansion of GAG-binding cells which migrate to anatomical sites rich in GAGs. These GAG-binding cells might, in turn, promote the inflammation and pathology seen both in our murine model and in human RA.
Figures
References
-
- Reichlin M. (2001) in Arthritis and Allied Conditions, ed. Koopman, W. (Lippincott, Philadelphia), pp. 1445–1479.
-
- Centers for Disease Control (2001) Morbid. Mortal. Wkly. Rep. 50, 120-125.
-
- Hale L. & Haynes, B. (2001) in Arthritis and Allied Conditions, ed. Koopman, W. (Lippincott, Philadelphia), pp. 1103–1127.
-
- Chakrabarti B. & Park, J. W. (1980) CRC Crit. Rev. Biochem. 8, 225-313. - PubMed
-
- Couchman J. (2001) in Arthritis and Allied Conditions, ed. Koopman, W. (Lippincott, Philadelphia), pp. 209–225.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
