

Interventions used in disease management programmes for patients with chronic illness-which ones work? Meta-analysis of published reports
- PMID: 12399340
- PMCID: PMC130055
- DOI: 10.1136/bmj.325.7370.925
Interventions used in disease management programmes for patients with chronic illness-which ones work? Meta-analysis of published reports
Abstract
Objective: To systematically evaluate the published evidence regarding the characteristics and effectiveness of disease management programmes.
Design: Meta-analysis.
Data sources: Computerised databases for English language articles during 1987-2001.
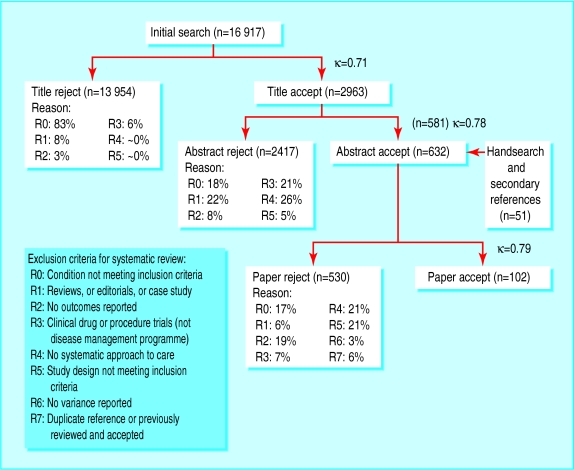
Study selection: 102 articles evaluating 118 disease management programmes.
Main outcome measures: Pooled effect sizes calculated with a random effects model.
Results: Patient education was the most commonly used intervention (92/118 programmes), followed by education of healthcare providers (47/118) and provider feedback (32/118). Most programmes (70/118) used more than one intervention. Provider education, feedback, and reminders were associated with significant improvements in provider adherence to guidelines (effect sizes (95% confidence intervals) 0.44 (0.19 to 0.68), 0.61 (0.28 to 0.93), and 0.52 (0.35 to 0.69) respectively) and with significant improvements in patient disease control (effect sizes 0.35 (0.19 to 0.51), 0.17 (0.10 to 0.25), and 0.22 (0.1 to 0.37) respectively). Patient education, reminders, and financial incentives were all associated with improvements in patient disease control (effect sizes 0.24 (0.07 to 0.40), 0.27 (0.17 to 0.36), and 0.40 (0.26 to 0.54) respectively).
Conclusions: All studied interventions were associated with improvements in provider adherence to practice guidelines and disease control. The type and number of interventions varied greatly, and future studies should directly compare different types of intervention to find the most effective.
Figures
Comment in
-
Care for chronic diseases.BMJ. 2002 Oct 26;325(7370):913-4. doi: 10.1136/bmj.325.7370.913. BMJ. 2002. PMID: 12399321 Free PMC article. No abstract available.
-
Unit of analysis errors should be clarified in meta-analyses.BMJ. 2003 Feb 15;326(7385):397. doi: 10.1136/bmj.326.7385.397. BMJ. 2003. PMID: 12586684 Free PMC article. No abstract available.
-
Review: most disease management programs for providers and patients lead to improvements in care.ACP J Club. 2003 Mar-Apr;138(2):55. ACP J Club. 2003. PMID: 12614140 No abstract available.
References
-
- Smith DH, Malone DC, Lawson KA, Okamoto LJ, Battista C, Saunders WB. A national estimate of the economic costs of asthma. Am J Respir Crit Care Med. 1997;156:787–793. - PubMed
-
- Greenberg PE, Stiglin LE, Finkelstein SN, Berndt ER. The economic burden of depression in 1990. J Clin Psychiatry. 1993;54:405–418. - PubMed
-
- American Diabetes Association. Economic consequences of diabetes mellitus in the US in 1997. Diabetes Care. 1998;21:296–309. - PubMed
-
- Ellrodt G, Cook DJ, Lee J, Cho M, Hunt D, Weingarten S. Evidence-based disease management. JAMA. 1997;278:1687–1692. - PubMed
-
- Epstein WA, Sanchez M, Kechijian P. Conjunctivitis. Arch Dermatol. 1985;121:838. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical