

A randomised controlled trial of patient self management of oral anticoagulation treatment compared with primary care management
- PMID: 12401823
- PMCID: PMC1769803
- DOI: 10.1136/jcp.55.11.845
A randomised controlled trial of patient self management of oral anticoagulation treatment compared with primary care management
Abstract
Background: The increase in numbers of patients receiving warfarin treatment has led to the development of alternative models of service delivery for oral anticoagulant monitoring. Patient self management for oral anticoagulation is a model new to the UK. This randomised trial was the first to compare routine primary care management of oral anticoagulation with patient self management.
Aim: To test whether patient self management is as safe, in terms of clinical effectiveness, as primary care management within the UK, as assessed by therapeutic international normalised ratio (INR) control.
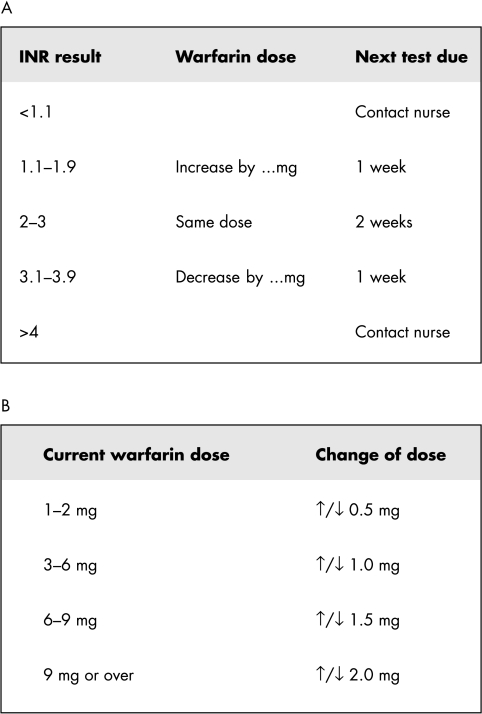
Method: Patients receiving warfarin from six general practices who satisfied study entry criteria were eligible to enter the study. Eligible patients were randomised to either intervention (patient self management) or control (routine primary care management) for six months. The intervention comprised two training sessions of one to two hours duration. Patients were allowed to undertake patient self management on successful completion of training. INR testing was undertaken using a Coaguchek device and regular internal/external quality control tests were performed. Patients were advised to perform INR tests every two weeks, or weekly if a dose adjustment was made. Dosage adjustment was undertaken using a simple dosing algorithm.
Results: Seventy eight of 206 (38%) patients were eligible for inclusion and, of these, 35 (45%) declined involvement or withdrew from the study. Altogether, 23 intervention and 26 control patients entered the study. There were no significant differences in INR control (per cent time in range: intervention, 74%; control, 77%). There were no serious adverse events in the intervention group, with one fatal retroperitoneal haemorrhage in the control group. Costs of patient self management were significantly greater than for routine care (pound 90 v pound 425/patient/year).
Conclusion: These are the first UK data to demonstrate that patient self management is as safe as primary care management for a selected population. Further studies are needed to elucidate whether this model of care is suitable for a larger population.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical