

Community-based exercise program reduces risk factors for falls in 65- to 75-year-old women with osteoporosis: randomized controlled trial
- PMID: 12403738
- PMCID: PMC134175
Community-based exercise program reduces risk factors for falls in 65- to 75-year-old women with osteoporosis: randomized controlled trial
Erratum in
- CMAJ. 2003 Jan 21;168(2):152.
Abstract
Background: Exercise programs improve balance, strength and agility in elderly people and thus may prevent falls. However, specific exercise programs that might be widely used in the community and that might be "prescribed" by physicians, especially for patients with osteoporosis, have not been evaluated. We conducted a randomized controlled trial of such a program designed specifically for women with osteoporosis.
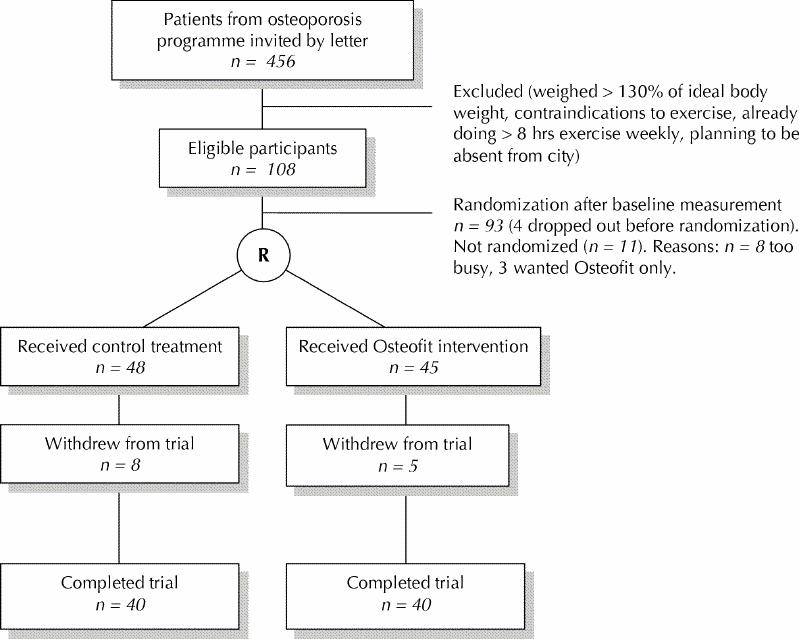
Methods: We identified women 65 to 75 years of age in whom osteoporosis had been diagnosed by dual-energy X-ray absorptiometry in our hospital between 1996 and 2000 and who were not engaged in regular weekly programs of moderate or hard exercise. Women who agreed to participate were randomly assigned to participate in a twice-weekly exercise class or to not participate in the class. We measured baseline data and, 20 weeks later, changes in static balance (by dynamic posturography), dynamic balance (by a timed figure-eight run) and knee extension strength (by dynamometry).
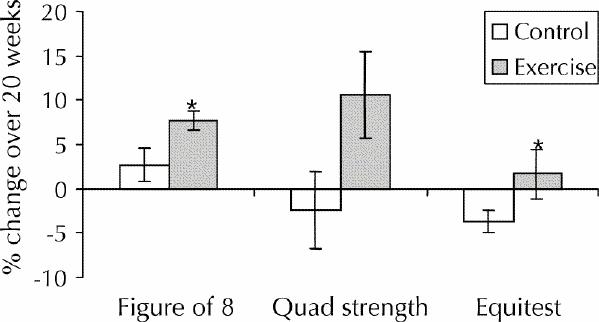
Results: Of 93 women who began the trial, 80 completed it. Before adjustment for covariates, the intervention group tended to have greater, although nonsignificant, improvements in static balance (mean difference 4.8%, 95% confidence interval [CI] -1.3% to 11.0%), dynamic balance (mean difference 3.3%, 95% CI -1.7% to 8.4%) and knee extension strength (mean difference 7.8%, 95% CI -5.4% to 21.0%). Mean crude changes in the static balance score were -0.85 (95% CI -2.91 to 1.21) for the control group and 1.40 (95% CI -0.66 to 3.46) for the intervention group. Mean crude changes in figure-eight velocity (dynamic balance) were 0.08 (95% CI 0.02 to 0.14) m/s for the control group and 0.14 (95% CI 0.08 to 0.20) m/s for the intervention group. For knee extension strength, mean changes were -0.58 (95% CI -3.02 to 1.81) kg/m for the control group and 1.03 (95% CI -1.31 to 3.34) kg/m for the intervention group. After adjustment for age, physical activity and years of estrogen use, the improvement in dynamic balance was 4.9% greater for the intervention group than for the control group (p = 0.044). After adjustment for physical activity, cognitive status and number of fractures ever, the improvement in knee extension strength was 12.8% greater for the intervention group than for the control group (p = 0.047). The intervention group also had a 6.3% greater improvement in static balance after adjustment for rheumatoid arthritis and osteoarthritis, but this difference was not significant (p = 0.06).
Interpretation: Relative to controls, participants in the exercise program experienced improvements in dynamic balance and strength, both important determinants of risk for falls, particularly in older women with osteoporosis.
Figures
Comment in
-
Preventing fractures by preventing falls in older women.CMAJ. 2002 Oct 29;167(9):1005-6. CMAJ. 2002. PMID: 12403739 Free PMC article. No abstract available.
References
-
- Close JCT, Glucksman E. Falls in the elderly: What can be done? Med J Aust 2000; 173:176-7. - PubMed
-
- Wolff I, van Croonenborg JJ, Kemper HCG, Kostense PJ, Twisk JWR. The effect of exercise training programs on bone mass: a meta-analysis of published controlled trials in pre- and postmenopausal women. Osteoporos Int 1999; 9:1-12. - PubMed
-
- Kelley G. Aerobic exercise and lumbar spine bone mineral density in postmenopausal women: a meta-analysis. J Am Geriatr Soc 1998;46(2):143-52. - PubMed
-
- Kelley GA, Kelley KS, Tran ZV. Resistance training and bone mineral density in women: a meta-analysis of controlled trials. Am J Phys Med Rehabil 2001; 80(1):65-77. - PubMed
-
- Kelley GA. Aerobic exercise and bone density at the hip in postmenopausal women: a meta-analysis. Prev Med 1998;27(6):798-807. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical