

Potential of surgery for curing type 2 diabetes mellitus
- PMID: 12409659
- PMCID: PMC1422611
- DOI: 10.1097/00000658-200211000-00003
Potential of surgery for curing type 2 diabetes mellitus
Abstract
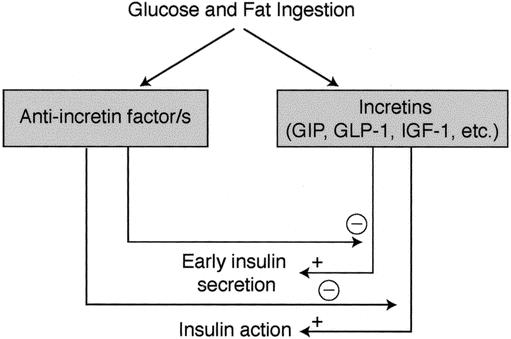
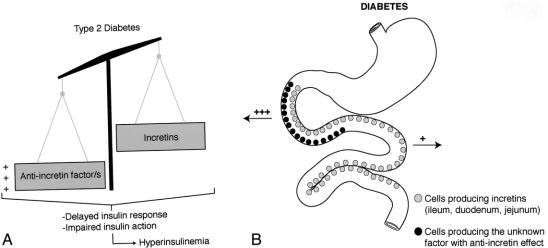
Objective: To review the effect of morbid obesity surgery on type 2 diabetes mellitus, and to analyze data that might explain the mechanisms of action of these surgeries and that could answer the question of whether surgery for morbid obesity can represent a cure for type 2 diabetes in nonobese patients as well.
Summary background data: Diabetes mellitus type 2 affects more than 150 million people worldwide. Although the incidence of complications of type 2 diabetes can be reduced with tight control of hyperglycemia, current therapies do not achieve a cure. Some operations for morbid obesity not only induce significant and lasting weight loss but also lead to improvements in or resolution of comorbid disease states, especially type 2 diabetes.
Methods: The authors reviewed data from the literature to address what is known about the effect of surgery for obesity on glucose metabolism and the endocrine changes that follow this surgery.
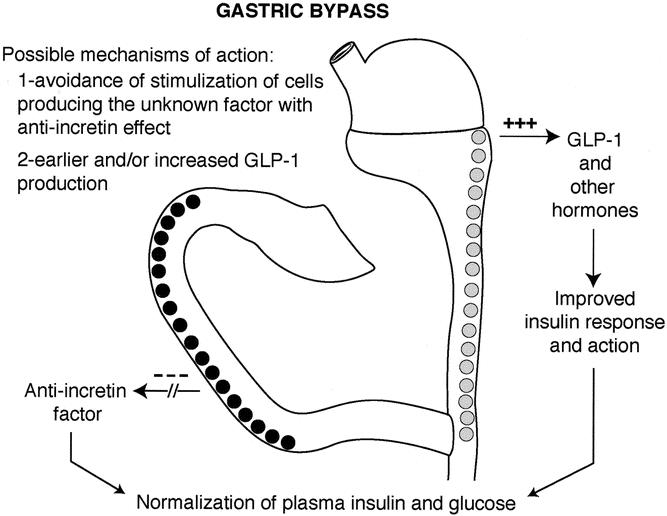
Results: Series with long-term follow-up show that gastric bypass and biliopancreatic diversion achieve durable normal levels of plasma glucose, plasma insulin, and glycosylated hemoglobin in 80% to 100% of severely obese diabetic patients, usually within days after surgery. Available data show a significant change in the pattern of secretion of gastrointestinal hormones. Case reports have also documented remission of type 2 diabetes in nonmorbidly obese individuals undergoing biliopancreatic diversion for other indications.
Conclusions: Gastric bypass and biliopancreatic diversion seem to achieve control of diabetes as a primary and independent effect, not secondary to the treatment of overweight. Although controlled trials are needed to verify the effectiveness on nonobese individuals, gastric bypass surgery has the potential to change the current concepts of the pathophysiology of type 2 diabetes and, possibly, the management of this disease.
Figures
References
-
- Venkat Narayan KM, Gregg EW, Fagot-Campagna A, et al. Diabetes: a common, growing, serious, costly, and potentially preventable public health problem. Diabetes Res Clin Pract 2000; 50 (Suppl 2): S77–84. - PubMed
-
- UK Prospective Diabetes Study Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPD 34). Lancet 1998; 352: 854–865. - PubMed
-
- Detournay B, Cros S, Charbonnel B, et al. Managing type 2 diabetes in France: the ECODIA survey. Diabetes Metab 2000; 26: 363–369. - PubMed
-
- Brolin RE. Update, NIH consensus conference, Gastrointestinal surgery for severe obesity. Nutrition 1996; 12: 403–404. - PubMed
-
- Gastrointestinal surgery for severe obesity. NIH consensus development conference, March 25–7, 1991. Nutrition 1996; 12:397–404. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
