

Hospital and surgeon procedure volume as predictors of outcome following rectal cancer resection
- PMID: 12409664
- PMCID: PMC1422616
- DOI: 10.1097/00000658-200211000-00008
Hospital and surgeon procedure volume as predictors of outcome following rectal cancer resection
Abstract
Objective: To compare surgeon and hospital procedure volume as predictors of outcomes for patients with rectal cancer.
Summary background data: Although a "volume-outcome" relationship exists for several major cancer operations, the impact of procedure volume on outcomes following rectal cancer surgery remains uncertain, and it has not been determined whether hospital or surgeon volume is a more important predictor of outcomes.
Methods: A retrospective population-based cohort study utilizing the Surveillance, Epidemiology and End Results (SEER)-Medicare linked database identified 2,815 rectal cancer patients aged 65 and older who had surgery for a primary tumor diagnosed in 1992-1996 in a SEER area. Hospital- and surgeon-specific procedure volume was ascertained based on the number of claims submitted over the 5-year study period. Outcome measures were mortality at 30 days and 2 years, overall survival, and the rate of abdominoperineal resections. Age, sex, race, comorbid illness, cancer stage, and socioeconomic status were used to adjust for differences in case mix.
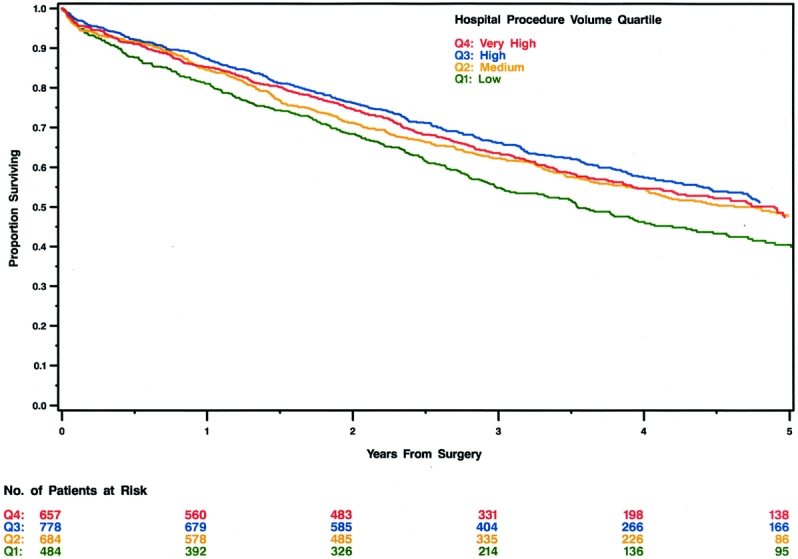
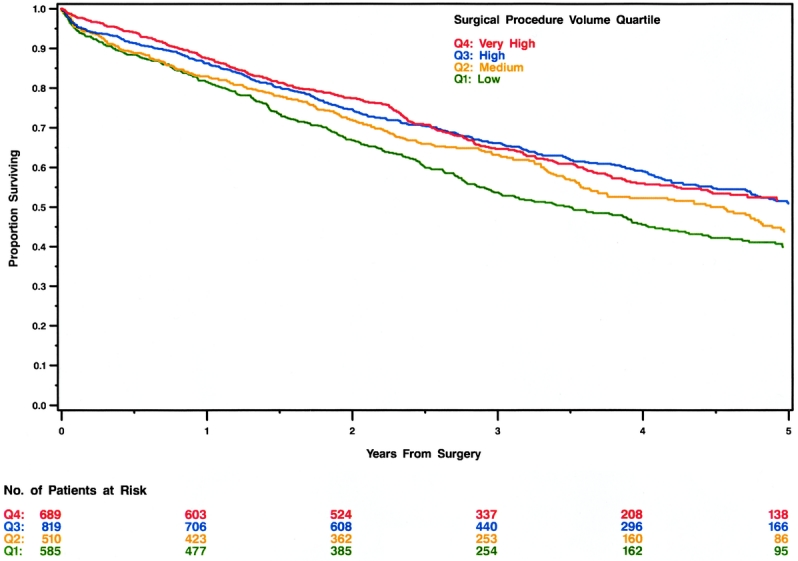
Results: Neither hospital- nor surgeon-specific procedure volume was significantly associated with 30-day postoperative mortality or rates of rectal sphincter-sparing operations. Although an association between hospital volume and mortality at 2 years was evident, this finding was no longer significant once surgeon-specific volume was controlled for. In contrast, surgeon-specific volume was associated with 2-year mortality and remained an important predictor even after adjustment for hospital volume. Surgeon volume was also better than hospital procedure volume at predicting long-term survival.
Conclusions: Surgeon-specific experience as measured by procedure volume can have a significant impact on survival for patients with rectal cancer.
Figures
References
-
- Hermanek P, Hohenberger W. The importance of volume in colorectal cancer surgery. Eur J Surg Oncol 1996; 22: 213–215. - PubMed
-
- Holm T, Johansson H, Cedermark B, et al. Influence of hospital- and surgeon-related factors on outcome after treatment of rectal cancer with or without preoperative radiotherapy. Br J Surg 1997; 84: 657–663. - PubMed
-
- Board NCP. Interpreting the volume–outcome relationship in the context of cancer care, Vol. 2001: http://www-iom.edu, 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
