

Extended hepatic resection for hepatocellular carcinoma in patients with cirrhosis: is it justified?
- PMID: 12409666
- PMCID: PMC1422618
- DOI: 10.1097/00000658-200211000-00010
Extended hepatic resection for hepatocellular carcinoma in patients with cirrhosis: is it justified?
Abstract
Objective: To evaluate the perioperative outcomes and long-term survival of extended hepatic resection for hepatocellular carcinoma (HCC) in patients with cirrhosis.
Summary background data: Hepatic resection is a well-established treatment for HCC in cirrhotic patients with preserved liver function and limited disease. However, the role of extended hepatic resection (more than four segments) for HCC in cirrhotic patients has not been elucidated.
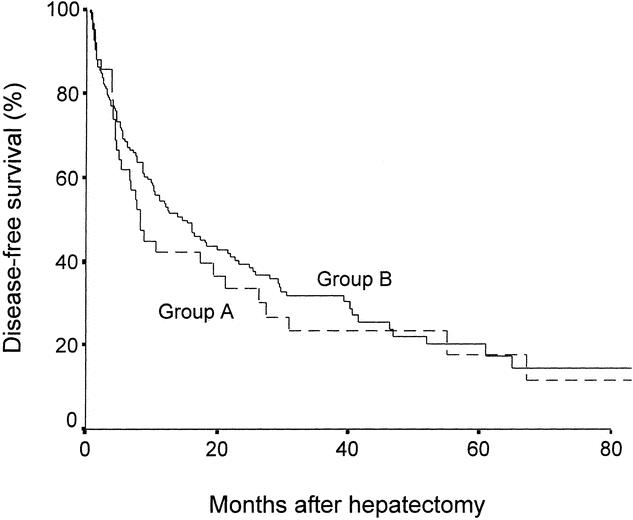
Methods: Between 1993 and 2000, 45 consecutive patients with histologically confirmed cirrhosis underwent right or left extended hepatectomy for HCC (group A). Perioperative outcomes and long-term survival of these patients were compared with 161 patients with HCC and cirrhosis who underwent hepatic resection of a lesser extent in the same period (group B). All clinicopathologic and follow-up data were collected prospectively.
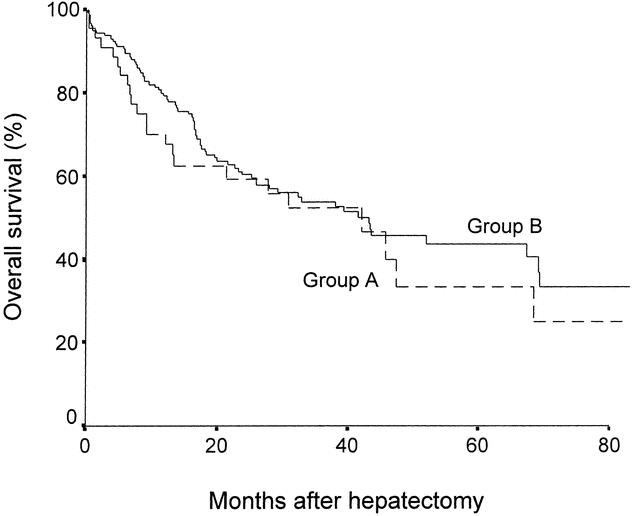
Results: Group A patients had significantly higher intraoperative blood loss, longer operation time, and longer hospital stay than group B. However, the two groups were similar in overall morbidity and hospital mortality. There were no significant differences in the incidence of liver failure or other complications. The resection margin width was similar between the two groups. Despite significantly larger tumor size in group A compared with group B, long-term survival was comparable between the two groups.
Conclusions: Extended hepatic resection for HCC can be performed in selected cirrhotic patients with acceptable morbidity, mortality, and long-term survival that are comparable to those of lesser hepatic resection. Extended hepatectomy for large HCC extending from one lobe to the other or central HCC critically related to the hepatic veins is justifiable in cirrhotic patients with preserved liver function and adequate liver remnant.
Figures
References
-
- Paquet KJ, Koussouris P, Mercado MA, et al. Limited hepatic resection for selected cirrhotic patients with hepatocellular or cholangiocellular carcinoma: a prospective study. Br J Surg 1991; 78: 459–462. - PubMed
-
- Capussotti L, Borgonovo G, Bouzari H, et al. Results of major hepatectomy for large primary liver cancer in patients with cirrhosis. Br J Surg 1994; 81: 427–431. - PubMed
-
- Fan ST, Lai ECS, Lo CM, et al. Hospital mortality of major hepatectomy for hepatocellular carcinoma associated with cirrhosis. Arch Surg 1995; 130: 198–203. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
