

Sporadic fundic gland polyps with epithelial dysplasia : evidence for preferential targeting for mutations in the adenomatous polyposis coli gene
- PMID: 12414520
- PMCID: PMC1850790
- DOI: 10.1016/S0002-9440(10)64450-1
Sporadic fundic gland polyps with epithelial dysplasia : evidence for preferential targeting for mutations in the adenomatous polyposis coli gene
Abstract
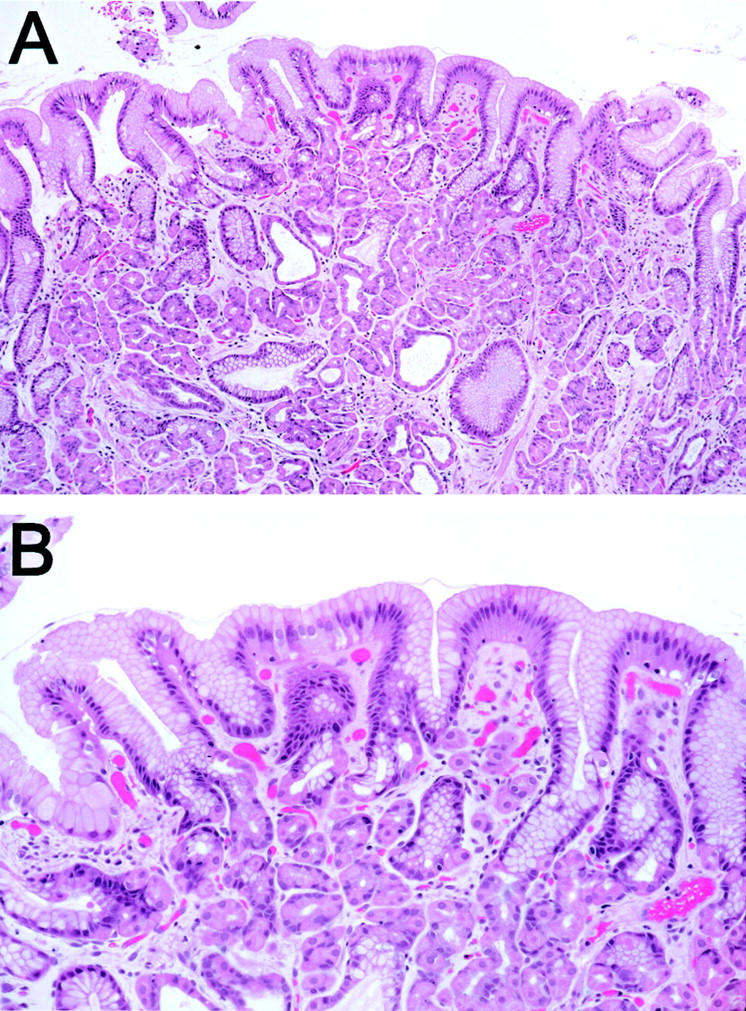
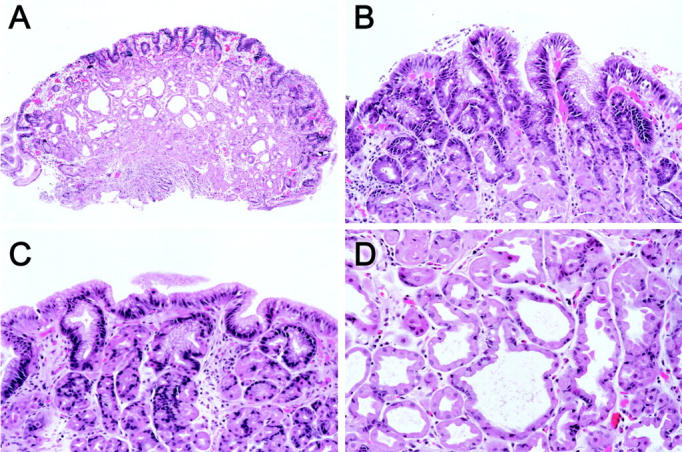
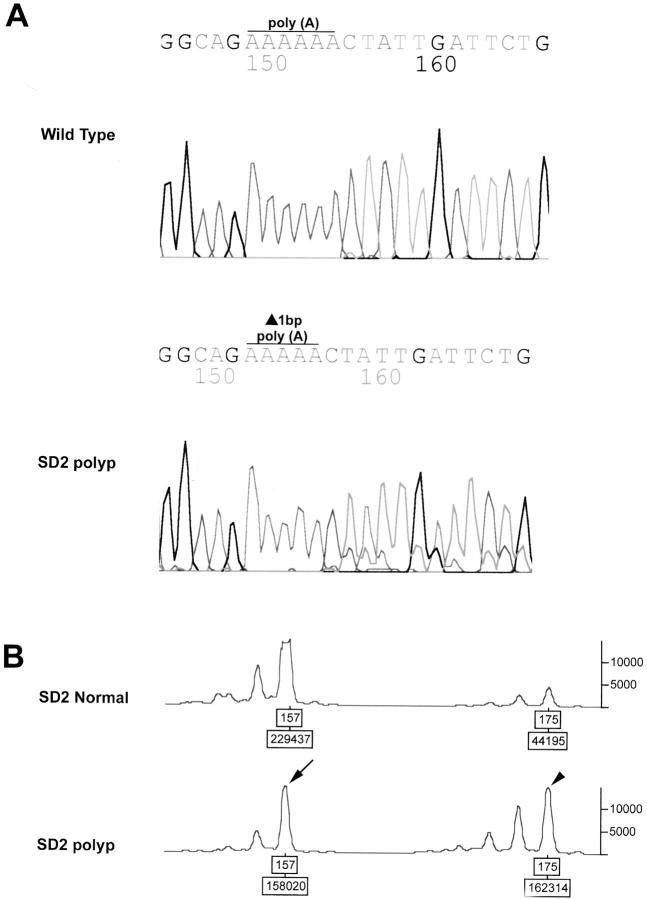
Gastric fundic gland polyps (FGPs) occur in two distinct clinicopathological scenarios: sporadic and familial adenomatous polyposis (FAP) associated. FAP-associated FGPs arise through somatic second hit alterations of the adenomatous polyposis coli (APC) gene and frequently demonstrate epithelial dysplasia (Am J Pathol 2000, 157:747-754). Sporadic FGPs, in contrast, tend to contain beta-catenin gene mutations and only infrequently show dysplasia (Am J Pathol 2001, 158:1005-1010). However, sporadic FGPs with dysplasia have not been previously investigated. We studied 13 sporadic FGPs with surface/foveolar low-grade dysplasia or changes indefinite for dysplasia for alterations in the APC/beta-catenin pathway, using chromosome 5q allelic loss assays and direct DNA sequencing of the mutation cluster region in exon 15 of APC and the phosphorylation region in exon 3 of beta-catenin. In addition, to evaluate for possible additional genetic alterations in FGPs, all cases were evaluated for microsatellite instability using fluorescent-based amplification of a standard panel of five microsatellite markers. Alterations in APC were present in seven (53.8%) FGPs, including two cases with bi-allelic APC inactivation (truncating intragenic mutation plus 5q allelic loss), two cases with APC mutation only, and three cases with 5q allelic loss only. In contrast, only two (15.4%) FGPs contained stabilizing beta-catenin mutations. All 13 FGPs were microsatellite stable. These results indicate that sporadic FGPs with dysplasia/indefinite for dysplasia are molecularly similar to FAP-associated FGPs, and are dissimilar to the more common sporadic nondysplastic FGPs. Mutations in APC and beta-catenin, despite occurring in the same genetic pathway, show differing biological properties, a phenomenon that has previously been demonstrated in colorectal neoplasms. The lack of microsatellite instability in FGPs in this study and of K-ras mutations in a previous study suggests that secondary genetic alterations are rare in both dysplastic and nondysplastic FGPs.
Figures

References
-
- Stolte M, Sticht T, Eidt S, Ebert D, Finkenzeller G: Frequency, location, and age and sex distribution of various types of gastric polyp. Endoscopy 1994, 26:659-665 - PubMed
-
- Sipponen P, Laxen F, Seppala K: Cystic ‘hamartomatous’ gastric polyps: a disorder of oxyntic glands. Histopathology 1983, 7:729-737 - PubMed
-
- Marcial MA, Villafana M, Hernandez-Denton J, Colon-Pagan JR: Fundic gland polyps: prevalence and clinicopathologic features. Am J Gastroenterol 1993, 88:1711-1713 - PubMed
-
- Kinoshita Y, Tojo M, Yano T, Kitajima N, Itoh T, Nishiyama K, Inatome T, Fukuzaki H, Watanabe M, Chiba T: Incidence of fundic gland polyps in patients without familial adenomatous polyposis. Gastrointest Endosc 1993, 39:161-163 - PubMed
-
- Iida M, Yao T, Itoh H, Watanabe H, Kohrogi N, Shigelmatsu A, Iwashita A, Fujishima M: Natural history of fundic gland polyposis in patients with familial adenomatosis coli/Gardner’s syndrome. Gastroenterology 1985, 89:1021-1025 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
