

Lymph nodes of patients with regional metastases from head and neck squamous cell carcinoma as a predictor of pathologic outcome: size changes at CT before and after radiation therapy
- PMID: 12427611
- PMCID: PMC8185832
Lymph nodes of patients with regional metastases from head and neck squamous cell carcinoma as a predictor of pathologic outcome: size changes at CT before and after radiation therapy
Abstract
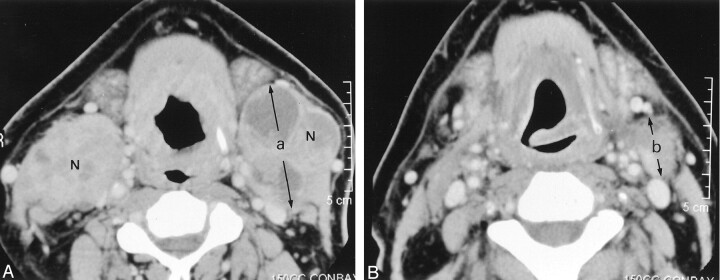
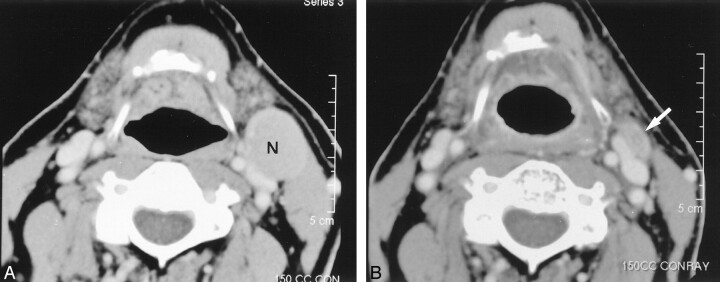
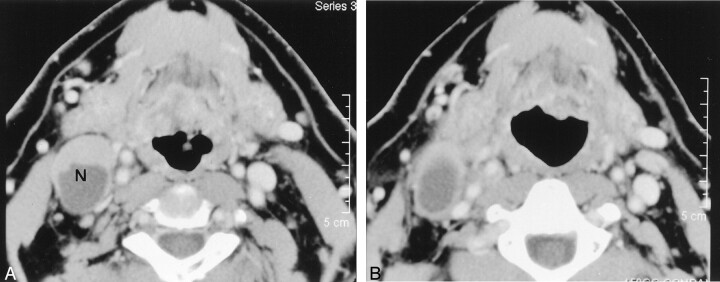
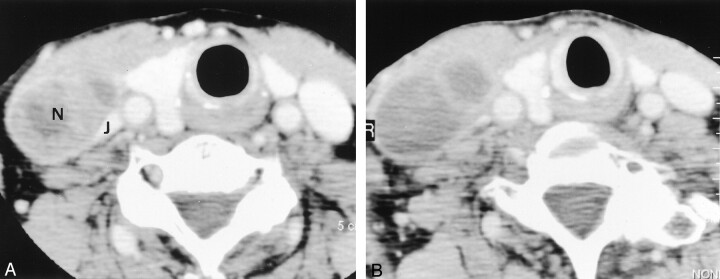
Background and purpose: Viable tumor in a neck dissection specimen is important in predicting prognosis and directing treatment. Our purpose was to clarify the importance of size changes of regional metastases from head and neck squamous cell carcinoma on CT scans obtained before and after radiation therapy (RT) as a predictor of pathologic outcome.
Methods: Thirty-seven heminecks in 34 patients who underwent pre-RT CT, RT, post-RT CT, and post-RT neck dissection were reviewed. Thirteen hemineck specimens were pathologically positive. Decrease ratios of the largest axial dimension of the lymph nodes between the pre- and post-RT CT studies were calculated.
Results: Six of 37 heminecks had a decrease ratio greater than 50%. These yielded negative specimens after planned neck dissection. In two of 37 heminecks, the largest axial dimension of the largest node increased between studies, resulting in negative decrease ratio. One (decrease ratio, -20%) had a positive specimen, and the other (decrease ratio, -3%) had a negative specimen. No interval change in size in the largest node was noted in one of the 37 heminecks; its specimen was positive. Average decrease ratios were 41.2% (range, -3% to 62%) in the negative specimen group (n = 24) and 27.2% (range, -20% to 50%) in the positive specimen group (n = 13). Univariate analysis revealed that the decrease ratio was not a significant predictor of a positive surgical specimen (P =.154).
Conclusion: Heminecks in which the decrease ratio was greater than 50% tended to have a negative surgical specimen. However, this trend was not statistically significant.
Figures
Comment in
-
Detection of residual disease of lymph node metastases in the neck, which is treated by (chemo)radiation.AJNR Am J Neuroradiol. 2002 Nov-Dec;23(10):1618-9. AJNR Am J Neuroradiol. 2002. PMID: 12427607 Free PMC article. No abstract available.
References
-
- Parsons JT, Mendenhall WM, Cassisi NJ, Stringer SP, Million RR. Neck dissection after twice-a-day radiotherapy: morbidity and recurrence rates. Head Neck 1989;11:400–404 - PubMed
-
- Mendenhall WM, Million RR, Cassisi NJ. Squamous cell carcinoma of the head and neck treated with radiation therapy: the role of neck dissection for clinically positive neck nodes. Int Radiat Oncol Biol Phys 1986;12:733–740 - PubMed
-
- Mabanta SR, Mendenhall WM, Stringer SP, Cassisi NJ. Salvage treatment for neck recurrence after irradiation alone for head and neck squamous cell carcinoma with clinically positive neck nodes. Head Neck 1999;21:591–594 - PubMed
-
- Boyd TS, Harai PM, Tannehill SP, et al. Planned postradiotherapy neck dissection in patients with advanced head and neck cancer. Head Neck 1998;20:132–137 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical