

Hepatopulmonary syndrome: prevalence and predictive value of various cut offs for arterial oxygenation and their clinical consequences
- PMID: 12427789
- PMCID: PMC1773478
- DOI: 10.1136/gut.51.6.853
Hepatopulmonary syndrome: prevalence and predictive value of various cut offs for arterial oxygenation and their clinical consequences
Abstract
Background: The hepatopulmonary syndrome (HPS) is defined as the triad of liver disease, arterial deoxygenation, and pulmonary vascular dilatation. The reported prevalence of HPS in cirrhotic patients varies between 4% and 19%, and various threshold values defining arterial deoxygenation have been used and recommended previously. However, it is not known how the prevalence of HPS differs using different cut off values for arterial deoxygenation.
Methods: We studied 127 patients for the presence of HPS using transthoracic contrast echocardiography for detection of pulmonary vasodilation, pulmonary function tests, and blood gas analysis.
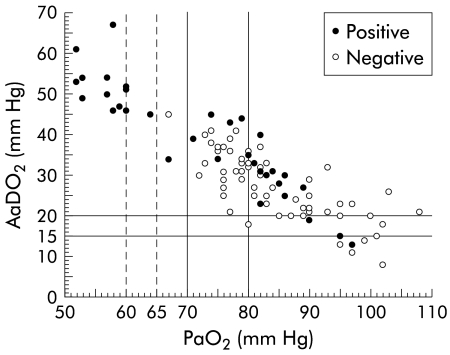
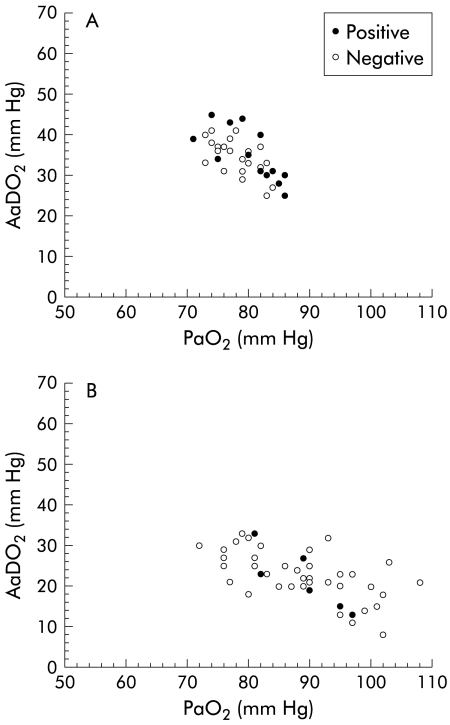
Results: Ninety eight patients were included in the study, of whom 33 (34%) had a positive contrast echocardiography. Using an increased alveolar-arterial difference for the partial pressure of oxygen (AaDO(2)) as an indication of hypoxaemia, the prevalence of HPS was considerably higher (>15 mm Hg, 32%; >20 mm Hg, 31%; and >age related threshold, 28%) than using reduced partial pressure of arterial oxygen (PaO(2)) as a threshold (<80 mm Hg, 19%; <70 mm Hg, 15%; and <age related threshold, 15%). For AaDO(2) as the cut off, the positive predictive value for a diagnosis of HPS was low (34%, 37%, and 53%, respectively). In contrast, PaO(2) as a cut off had considerably higher positive predictive values (44%, 93%, and 94%, respectively). Introducing PaO(2) <65 mm Hg as the cut off, the positive predictive value increased to 100%. Dyspnoea was more often present in patients with "clinically significant" HPS (57%) compared with "subclinical HPS" (8%), and patients without HPS (6%). The Child-Pugh score correlated significantly with the severity of HPS. Two of five liver transplanted patients with "subclinical HPS" had embolic brain infarcts, possibly induced by venous emboli passing through dilated intrapulmonary vessels.
Conclusions: Defining arterial hypoxaemia in HPS by different, previously used, cut off values for arterial oxygenation leads to a wide variation in the prevalence of HPS in the same sample of cirrhotic patients.
Figures
References
-
- Krowka MJ, Cortese DA. Hepatopulmonary syndrome. Current concepts in diagnostic and therapeutic considerations. Chest 1994;105:1528–37. - PubMed
-
- Lange PA, Stoller JK. The hepatopulmonary syndrome. Ann Intern Med 1995;122:521–9. - PubMed
-
- Krowka MJ. Hepatopulmonary syndrome. In: Plevak D, Seeff L, eds. Critical care issues in liver transplantation: The American Association for the Study of the Liver and the International Liver Transplantation Society; 1999:58–65.
-
- Abrams GA, Jaffe CC, Hoffer PB, et al. Diagnostic utility of contrast echocardiography and lung perfusion scan in patients with hepatopulmonary syndrome. Gastroenterology 1995;109:1283–8. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources