

Adoptive T cell therapy using antigen-specific CD8+ T cell clones for the treatment of patients with metastatic melanoma: in vivo persistence, migration, and antitumor effect of transferred T cells
- PMID: 12427970
- PMCID: PMC138583
- DOI: 10.1073/pnas.242600099
Adoptive T cell therapy using antigen-specific CD8+ T cell clones for the treatment of patients with metastatic melanoma: in vivo persistence, migration, and antitumor effect of transferred T cells
Abstract
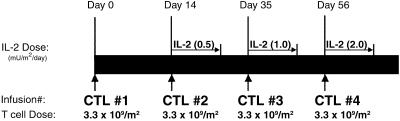
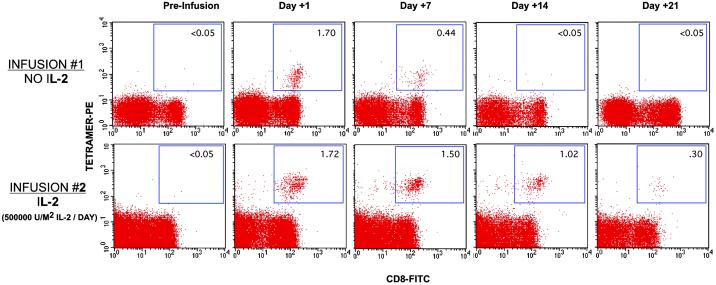
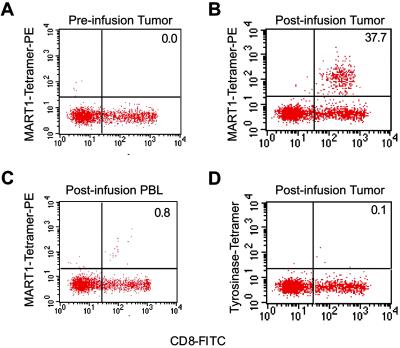
Adoptive T cell therapy, involving the ex vivo selection and expansion of antigen-specific T cell clones, provides a means of augmenting antigen-specific immunity without the in vivo constraints that can accompany vaccine-based strategies. A phase I study was performed to evaluate the safety, in vivo persistence, and efficacy of adoptively transferred CD8+ T cell clones targeting the tumor-associated antigens, MART1MelanA and gp100 for the treatment of patients with metastatic melanoma. Four infusions of autologous T cell clones were administered, the first without IL-2 and subsequent infusions with low-dose IL-2 (at 0.25, 0.50, and 1.0 x 10(6) unitsm(2) twice daily for the second, third, and fourth infusions, respectively). Forty-three infusions of MART1MelanA-specific or gp100-specific CD8+ T cell clones were administered to 10 patients. No serious toxicity was observed. We demonstrate that the adoptively transferred T cell clones persist in vivo in response to low-dose IL-2, preferentially localize to tumor sites and mediate an antigen-specific immune response characterized by the elimination of antigen-positive tumor cells, regression of individual metastases, and minor, mixed or stable responses in 8 of 10 patients with refractory, metastatic disease for up to 21 mo.
Figures



Comment in
-
T cells take aim at cancer.Proc Natl Acad Sci U S A. 2002 Dec 10;99(25):15840-2. doi: 10.1073/pnas.262669499. Epub 2002 Dec 2. Proc Natl Acad Sci U S A. 2002. PMID: 12461164 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
