

Early prediction of improvement in ejection fraction after acute myocardial infarction using low dose dobutamine echocardiography
- PMID: 12433887
- PMCID: PMC1767449
- DOI: 10.1136/heart.88.6.592
Early prediction of improvement in ejection fraction after acute myocardial infarction using low dose dobutamine echocardiography
Abstract
Objective: To evaluate the relation between changes in ejection fraction during the first three months after acute myocardial infarction and myocardial viability.
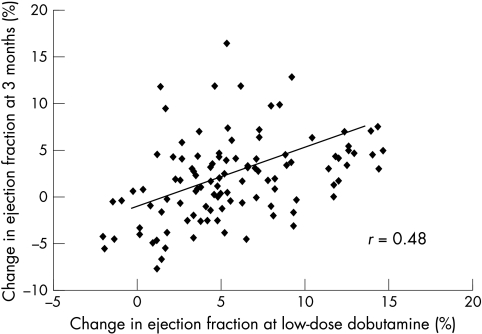
Patients: Myocardial viability was assessed using low dose dobutamine echocardiography in 107 patients at mean (SD) 3 (1) days after acute myocardial infarction. Cross sectional echocardiography was repeated three months later. Left ventricular volumes and ejection fraction were determined from apical views using the Simpson biplane formula.
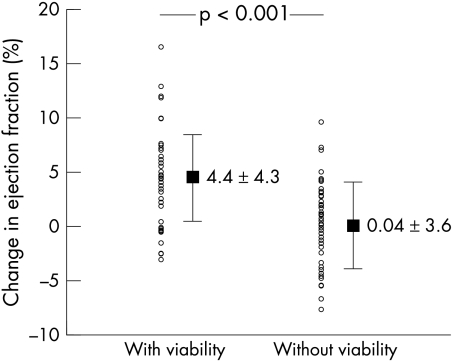
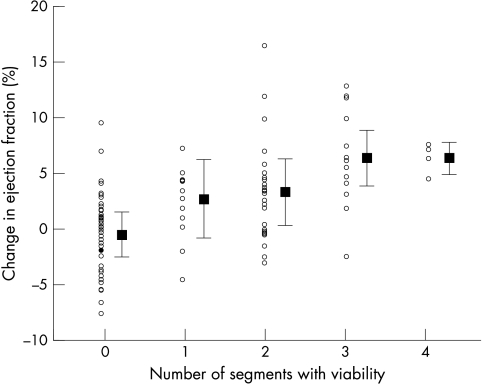
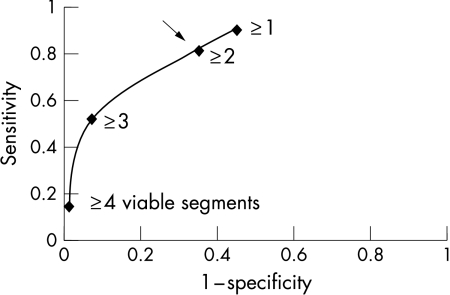
Results: In patients with viability, ejection fraction increased by 4.4 (4.3)%; in patients without viability it remained unchanged (0.04 (3.6)%; p < 0.001). A > or = 5% increase in ejection fraction was present in 21 of 107 patients (20%). Receiver operating characteristic analysis showed that myocardial viability in > or = 2 segments predicted this increase in ejection fraction with a sensitivity of 81% and a specificity of 65%. Multivariate logistic regression analysis was used to define which clinical and echocardiographic variables were related to > or = 5% improvement in ejection fraction. Myocardial viability, non-Q wave infarction, and anterior infarction all emerged as independent predictors, myocardial viability being the best (chi(2) = 14.5; p = 0.0001). Using the regression equation, the probability of > or = 5% improvement in ejection fraction for patients with a non-Q wave anterior infarct with viability was 73%, and for patients with a Q wave inferior infarct without viability, only 2%.
Conclusions: Myocardial viability after acute myocardial infarction is the single best predictor of improvement in ejection fraction. In combination with infarct location and Q wave presence, the probability of > or = 5% improvement can be estimated in individual patients at the bedside.
Figures
Comment in
-
Measuring left ventricular volume and ejection fraction with the biplane Simpson's method.Heart. 2002 Dec;88(6):559-60. doi: 10.1136/heart.88.6.559. Heart. 2002. PMID: 12433875 Free PMC article. No abstract available.
References
-
- The Multicenter Postinfarction Research Group. Risk stratification and survival after myocardial infarction. N Engl J Med 1983;309:331–6. - PubMed
-
- Volpi A, De Vita C, Franzosi MG, et al and the ad hoc Working Group of the Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico (GISSI)-2 data base. Determinants of 6-month mortality in survivors of myocardial infarction after thrombolysis. Results of the GISSI-2 data base. Circulation 1993;88:416–29. - PubMed
-
- Stadius ML, Davis K, Maynard C, et al. Risk stratification for 1 year survival based on characteristics identified in the early hours of acute myocardial infarction. The Western Washington Intracoronary Streptokinase Trial. Circulation 1986;74:703–11. - PubMed
-
- Sheehan FH, Braunwald E, Canner P, et al. The effect of intravenous thrombolytic therapy on left ventricular function: a report on tissue-type plasminogen activator and streptokinase from the thrombolysis in myocardial infarction (TIMI phase I) trial. Circulation 1987:75:817–29. - PubMed
-
- The TIMI Study Group. Comparison of invasive and conservative strategies after treatment with intravenous tissue plasminogen activator in acute myocardial infarction. Results of the thrombolysis in myocardial infarction (TIMI) phase II trial. N Engl J Med 1989;320:618–27. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical