

Review
doi: 10.1136/heart.88.6.665.
Myotonic dystrophy and the heart
Affiliations
- PMID: 12433913
- PMCID: PMC1767476
- DOI: 10.1136/heart.88.6.665
Item in Clipboard
Review
Myotonic dystrophy and the heart
Heart.
2002 Dec.
No abstract available
Figures
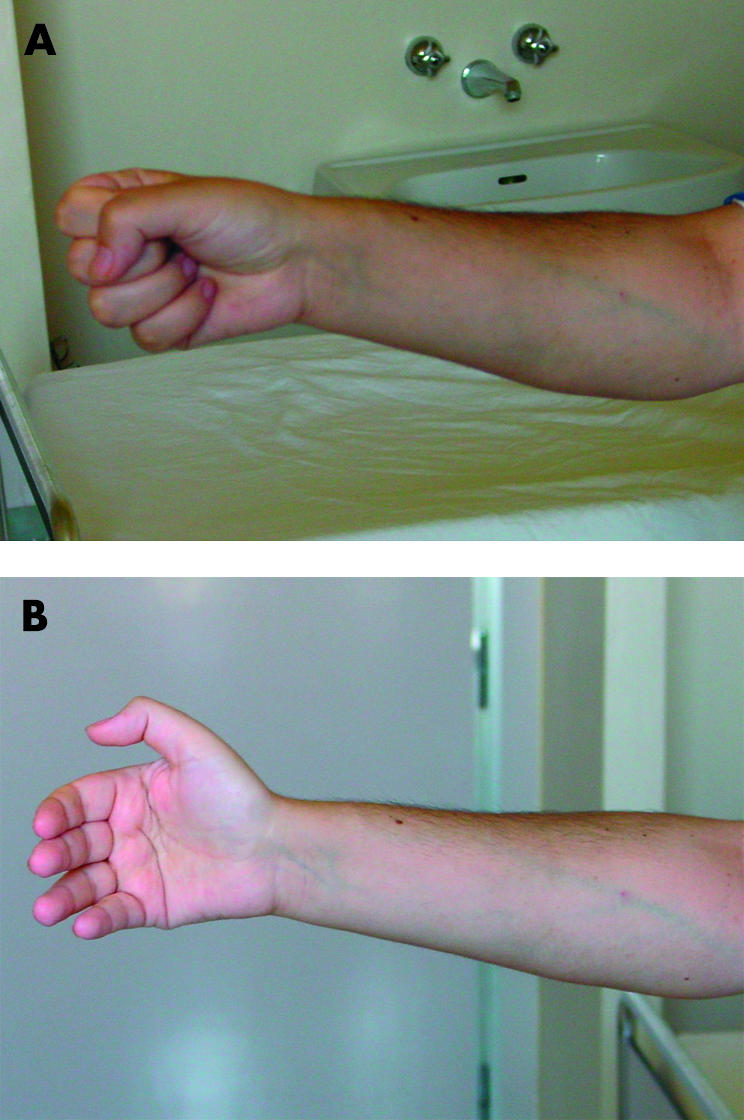
The grip test is a quick and easy way to determine the presence of active myotonia. After contraction of the fist (A) the patient is unable to relax the muscles of the hand (B). Photographs courtesy of Dr Gabriella Silvestri, Unione Italiana Lotta alla Distrofia Muscolare, Sezione Lazio, Italy.
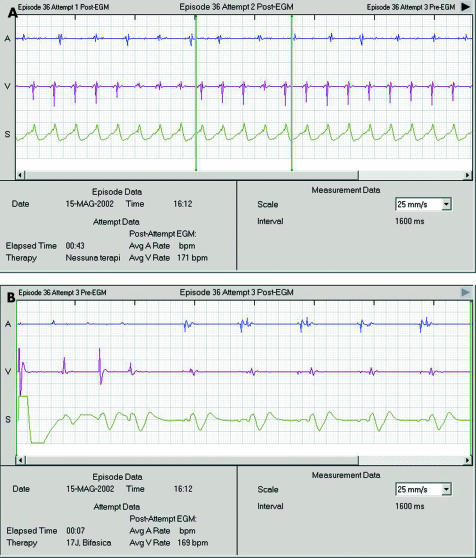
(A) Intracardiac electrograms (EGM) of a spontaneous episode of sustained ventricular tachycardia as recorded from the cardioverter-defibrillator (ICD) implanted in a 32 year old male patient affected by DM1. From top to bottom the tracings show the atrial EGM, the ventricular EGM, and a pseudo-surface lead II derived from signals recorded between the shock coils and the ICD. Atrioventricular dissociation, enabling a diagnosis of ventricular tachycardia, is evident. (B) Resumption of sinus rhythm after a 17 J biphasic DC shock.
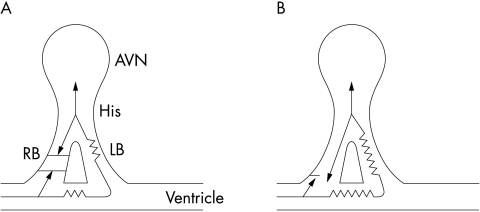
Bundle branch re-entry. (A) A ventricular premature impulse is blocked retrogradely in the right bundle branch (RB); conduction proceeds retrogradely through the left bundle branch (LB) up to the His bundle (His); from the His bundle, the impulse travels anterogradely over the right bundle branch which is still refractory, thus blocking propagation. (B) Conversely, if the right bundle branch has enough time to recover, the impulse can be conducted anterogradely to the ventricles, then retrogradely through the left bundle branch up to the His bundle, thus maintaining a macro-reentry. AVN, atrioventricular node.
References
-
- Mathieu J, Allard P, Potvin L, et al. A 10 year study of mortality in a cohort of patients with myotonic dystrophy. Neurology 1999;52:1658–62. ▸ This is a recent longitudinal study involving a large population of DM patients, followed for 10 years, which extensively investigates the natural history and the causes of death associated with the disease. - PubMed
-
- Melacini P, Villanova C, Menegazzo E, et al. Correlation between cardiac involvement and CTG trinucleotide repeat length in myotonic dystrophy. J Am Coll Cardiol 1995;25:239–45. ▸ This excellent work points out the possible predictive value of CTG repeats size on cardiac conduction abnormalities and their severity, adding also important information on the role of late potentials in predicting VT. - PubMed
-
- Saba S, Vanderbrink BA, Luciano B, et al. Localization of the sites of conduction abnormalities in a mouse model of myotonic dystrophy. J Cardiovasc Electrophysiol 1999;10:1214–20. ▸ This is one of the few experimental control studies in a mouse model of DM where affected mice underwent complete EPS, showing the higher predilection to the infrahissian tissue for conduction abnormalities related to DMPK loss. - PubMed
-
- Jaspert A, Fahsold R, Grehl, et al. Myotonic dystrophy correlation of clinical symptoms with the size of CTG repeats. J Neurol 1995;25:239–45. - PubMed
-
- Groh W, Lowe M, Zipes D. Severity of cardiac conduction involvement and arrhythmias in myotonic dystrophy type 1 correlates with age and CTG repeat length. J Cardiovasc Electrophysiol 2002;13:444–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical