

Target organ localization of memory CD4(+) T cells in patients with chronic beryllium disease
- PMID: 12438445
- PMCID: PMC151812
- DOI: 10.1172/JCI15846
Target organ localization of memory CD4(+) T cells in patients with chronic beryllium disease
Abstract
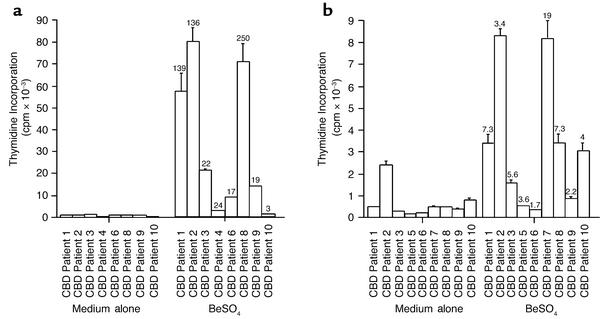
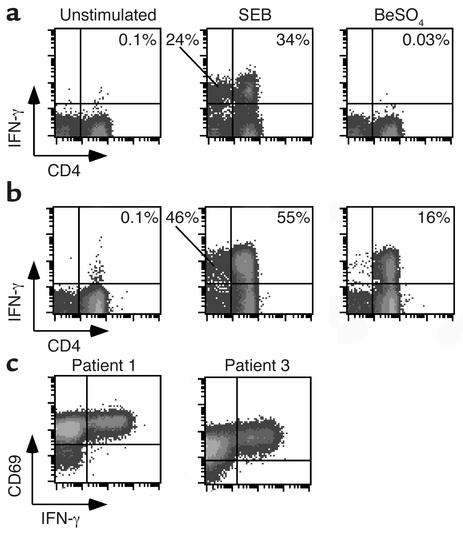
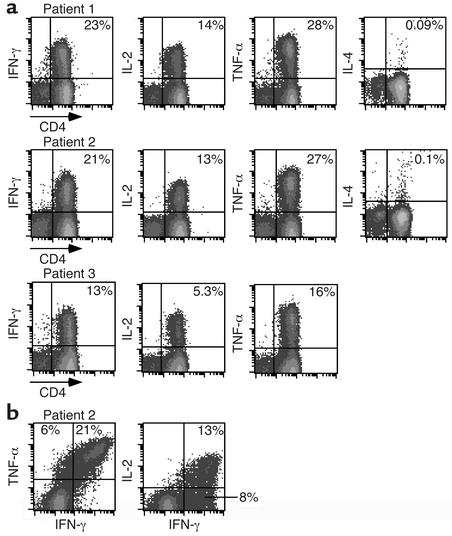
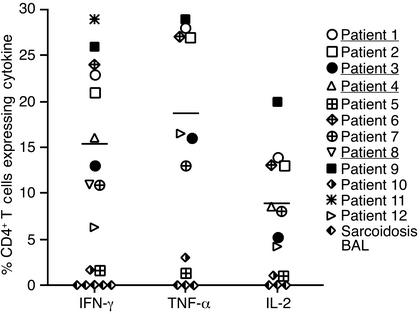
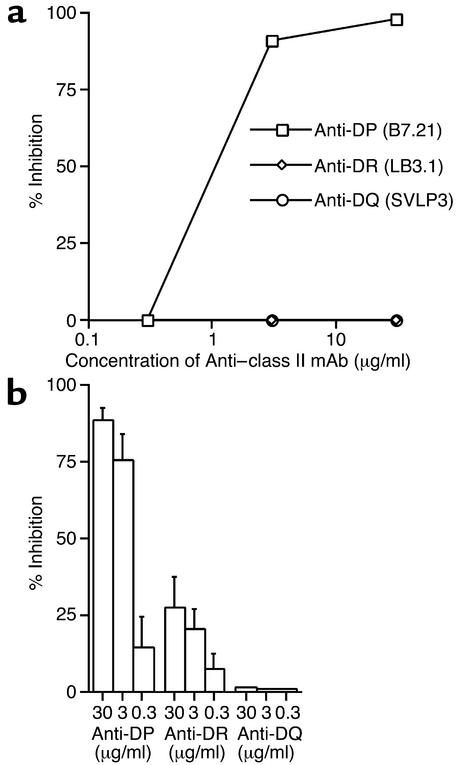
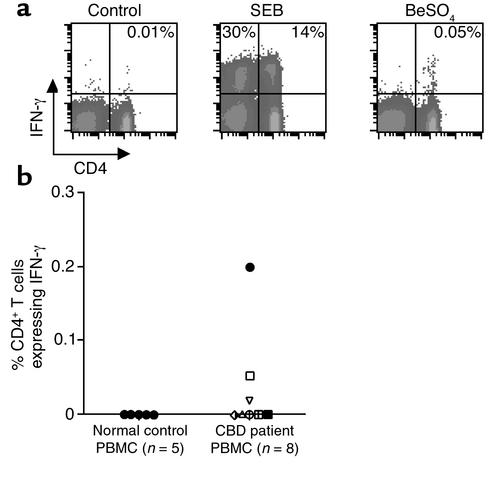
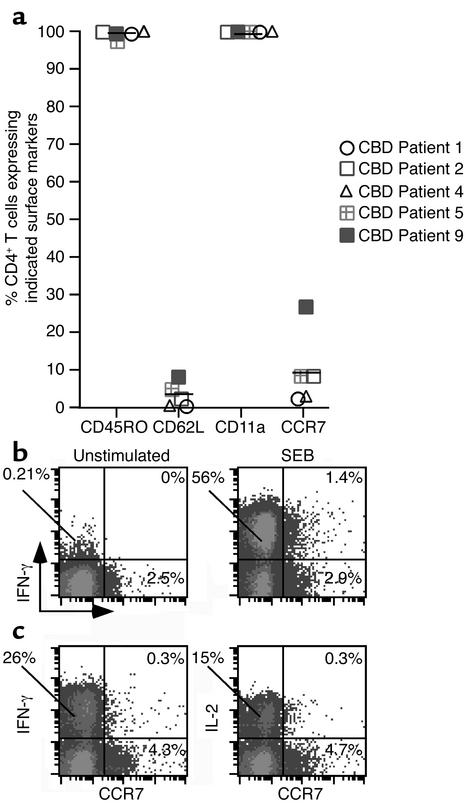
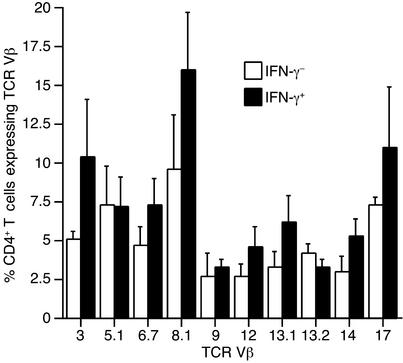
Chronic beryllium disease (CBD) is caused by exposure to beryllium in the workplace, and it remains an important public health concern. Evidence suggests that CD4(+) T cells play a critical role in the development of this disease. Using intracellular cytokine staining, we found that the frequency of beryllium-specific CD4(+) T cells in the lungs (bronchoalveolar lavage) of 12 CBD patients ranged from 1.4% to 29% (mean 17.8%), and these T cells expressed a Th1-type phenotype in response to beryllium sulfate (BeSO(4)). Few, if any, beryllium-specific CD8(+) T cells were identified. In contrast, the frequency of beryllium-responsive CD4(+) T cells in the blood of these subjects ranged from undetectable to 1 in 500. No correlation was observed between the frequency of beryllium-responsive bronchoalveolar lavage (BAL) CD4(+) T cells as detected by intracellular staining and lymphocyte proliferation in culture after BeSO(4) exposure. Staining for surface marker expression showed that nearly all BAL T cells exhibit an effector memory cell phenotype. These results demonstrate a dramatically high frequency and compartmentalization of antigen-specific effector memory CD4(+) cells in the lungs of CBD patients. These studies provide insight into the phenotypic and functional characteristics of antigen-specific T cells invading other inaccessible target organs in human disease.
Figures
References
-
- Newman, L.S., Maier, L.A., and Nemery, B. 1998. Interstitial lung disorders due to beryllium and cobalt. In Interstitial lung disease. M.I. Schwarz and T.E. King, Jr., editors. B.C. Decker Inc. Hamilton, Ontario. 367–392.
-
- Fontenot AP, Newman LS, Kotzin BL. Chronic beryllium disease: T cell recognition of a metal presented by HLA-DP. Clin Immunol. 2001;100:4–14. - PubMed
-
- Kreiss K, Wasserman S, Mroz MM, Newman LS. Beryllium disease screening in the ceramics industry: blood test performance and exposure-disease relations. J Occup Med. 1993;35:267–274. - PubMed
-
- Kreiss K, Mroz MM, Zhen B, Martyny JW, Newman LS. Epidemiology of beryllium sensitization and disease in nuclear workers. Am Rev Respir Dis. 1993;148:985–991. - PubMed
-
- Kreiss K, Mroz MM, Newman LS, Martyny J, Zhen B. Machining risk of beryllium disease and sensitization with median exposures below 2 μg/m3. Am J Ind Med. 1996;30:16–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
