

The risks of waiting for cardiac catheterization: a prospective study
- PMID: 12451076
- PMCID: PMC134132
The risks of waiting for cardiac catheterization: a prospective study
Erratum in
- CMAJ. 2003 Jan 21;168(2):152.
- CMAJ. 2003 Jun 10;168(12):1529
Abstract
Background: Few large, systematic, prospective studies have documented the characteristics and clinical outcomes of patients awaiting cardiac catheterization and the delays that they experience. The primary objective of this study was to quantify the waiting times, morbidity and mortality of patients waiting for catheterization. A secondary objective was to identify predictors of cardiac events that occur while patients are waiting.
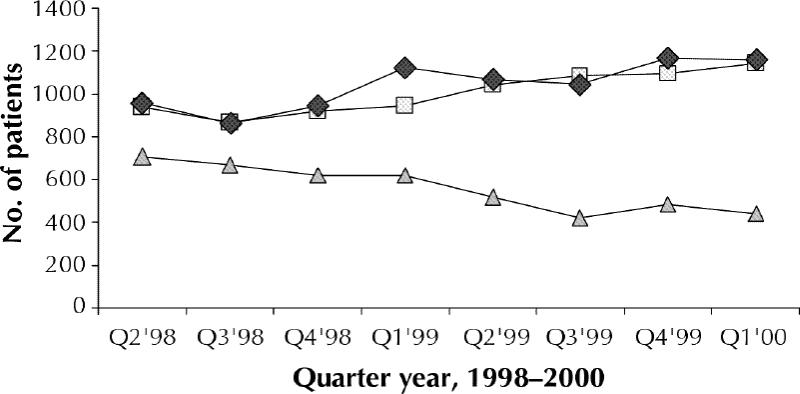
Methods: A computerized, prospective, central waiting list registry was developed at a regional centre in Hamilton, Ont., serving 2.2 million people in southern Ontario. Between Apr. 1, 1998, and Mar. 31, 2000, 8030 consecutive patients (4725 outpatients and 3305 inpatients) were referred for cardiac catheterization. Major cardiac outcomes while on the waiting list (death, myocardial infarction and congestive heart failure) were documented prospectively and related to requested versus actual waiting time.
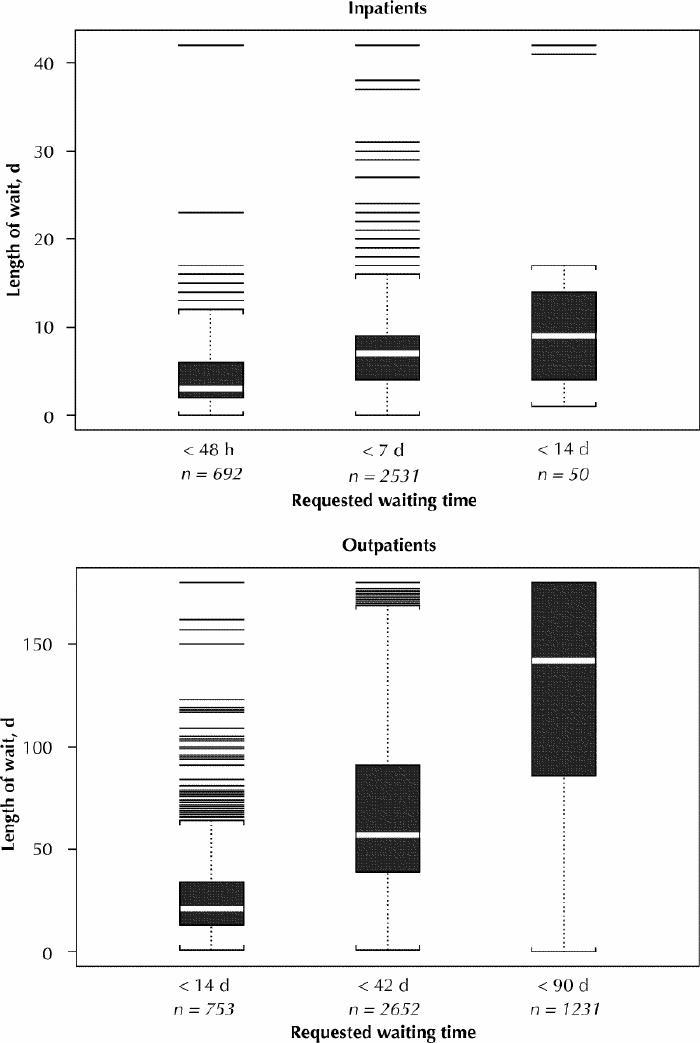
Results: Most of the referrals (7345 [91.5%]) were for a primary diagnosis of suspected coronary artery disease. The median waiting time was 6 (interquartile range [IQR] 4) days for inpatients and 60 (IQR 68) days for outpatients. Actual waiting times correlated with the waiting times requested by the referring physicians. However, only 37% of the procedures overall were completed within the requested waiting time. Of the 8030 patients, 50 (0.6%) died, 32 (0.4%) had a myocardial infarction and 41 (0.5%) experienced congestive heart failure. Overall, 109 patients (1.4%) had a major cardiac event, namely, death, myocardial infarction or congestive heart failure. These events occurred over a median wait of 27 days (2 days for inpatients and 35 days for outpatients), and over half (57%) occurred within the waiting time requested by the referring physician. In the multivariate analysis, predictors of the composite of death, myocardial infarction or congestive heart failure were increasing age (relative risk [RR] 2.39, 95% confidence interval [CI] 1.52-3.75) and New York Heart Association class III/IV symptoms (RR 2.86, 95% CI 1.11-7.33) in inpatients, and increasing age (RR 1.36, 95% CI 1.12-1.66), aortic stenosis (RR 3.70, 95% CI 1.93-7.08) and left ventricular ejection fraction less than 35% (RR 4.35, 95% CI 2.48-7.61) in outpatients.
Interpretation: Patients awaiting cardiac catheterization may experience major adverse events, such as death, myocardial infarction and congestive heart failure, which may be preventable. Our findings provide a benchmark by which to measure the effect of increased capacity and prioritization schemes that allow earlier access for patients at higher risk, such as those with aortic stenosis and reduced left ventricular function.
Figures
Comment in
-
The waiting game: facing the consequences.CMAJ. 2002 Nov 26;167(11):1247-8. CMAJ. 2002. PMID: 12451078 Free PMC article. No abstract available.
-
Relative risks or odds ratios?CMAJ. 2003 Jun 10;168(12):1529; author reply 1529. CMAJ. 2003. PMID: 12796330 Free PMC article. No abstract available.
References
-
- Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, et al. ACC/AHA guidelines for coronary angiography. J Am Coll Cardiol 1999;33: 1756-824. - PubMed
-
- Higginson LA, Naylor CD. Rates of cardiac catheterization, coronary angioplasty and coronary artery bypass surgery in Canada. Can J Cardiol 1997;13 (Suppl D):47D-52D. - PubMed
-
- Naylor CD, Sykora K, Jaglal SB, Jefferson S. Waiting for coronary artery bypass surgery: population-based study of 8517 consecutive patients in Ontario, Canada. The Steering Committee of the Adult Cardiac Care Network of Ontario. Lancet 1995;346:1605-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous