

A decade of experience with renal transplantation in African-Americans
- PMID: 12454518
- PMCID: PMC1422646
- DOI: 10.1097/00000658-200212000-00012
A decade of experience with renal transplantation in African-Americans
Abstract
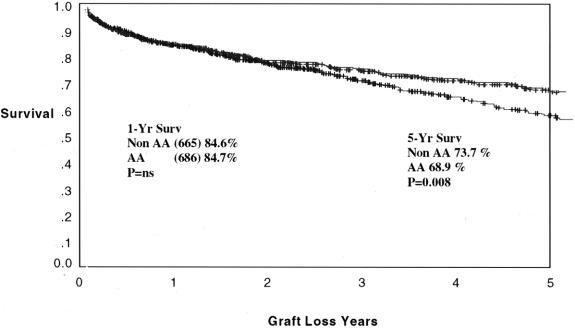
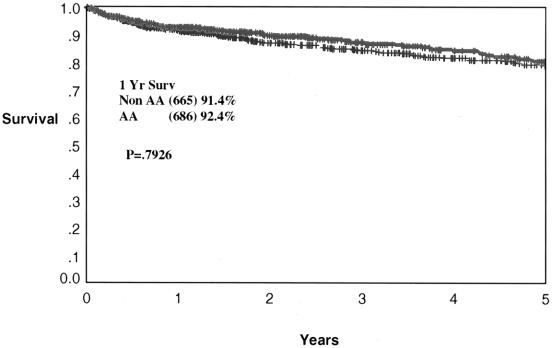
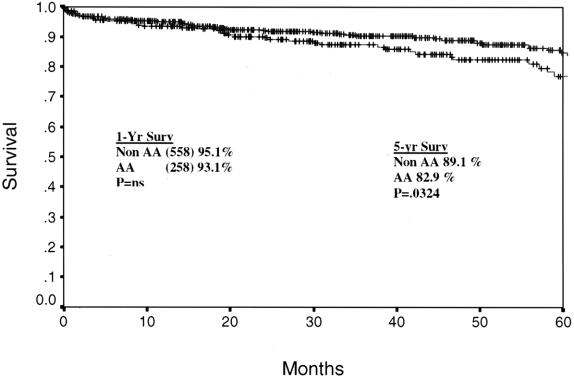
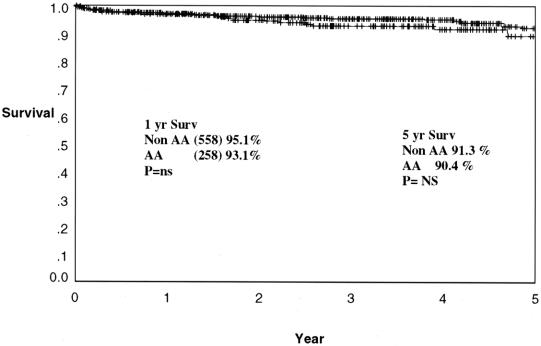
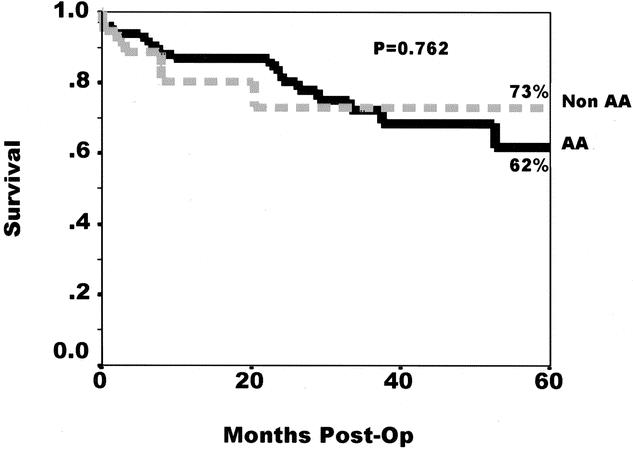
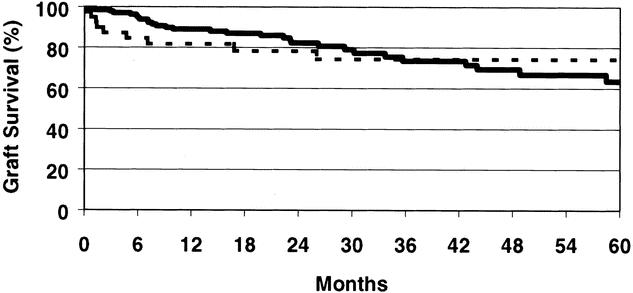
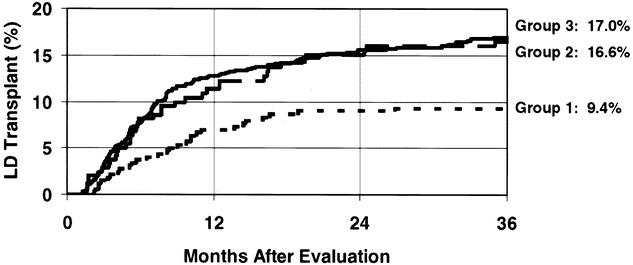
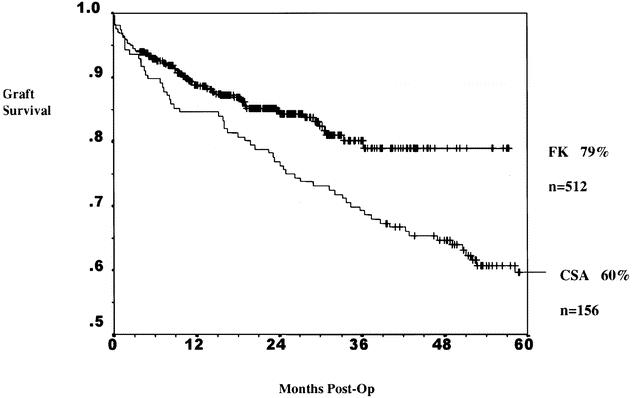
OBJECTIVE To evaluate the strategies instituted by the authors' center to decrease the time to transplantation and increase the rate of transplantation for African-Americans, consisting of a formal education program concerning the benefits of living organ donation that is oriented to minorities; a laparoscopic living donation program; use of hepatitis C-positive donors in documented positive recipients; and encouraging vaccination for hepatitis B, allowing the use of hepatitis B core Ab-positive donors. SUMMARY BACKGROUND DATA The national shortage of suitable kidney donor organs has disproportional and adverse effects on African-Americans for several reasons. Type II diabetes mellitus and hypertension, major etiologic factors for end-stage renal disease, are more prevalent in African-Americans than in the general population. Once kidney failure has developed, African-Americans are disadvantaged for the following reasons: this patient cohort has longer median waiting times on the renal transplant list; African-Americans have higher rates of acute rejection, which affects long-term allograft survival; and once they are transplanted, the long-term graft survival rates are lower in this population than in other groups. METHODS From March 1990 to November 2001 the authors' center performed 2,167 renal transplants; 944 were in African-Americans (663 primary cadaver renal transplants and 253 primary Living donor renal transplants). The retransplants consisted of 83 cadaver transplants and 17 living donor transplants. Outcome measures of this retrospective analysis included median waiting time, graft and patient survival rates, and the rate of living donation in African-Americans and comparable non-African-Americans. Where applicable, data are compared to United Network for Organ Sharing national statistics. Statistical analysis employed appropriate SPSS applications. RESULTS One- and 5-year patient survival rates for living donor kidneys were 97.1% and 91.3% for non-African-Americans and 96.8% and 90.4% for African-Americans. One- and 5-year graft survival rates were 95.1% and 89.1% for non-African-Americans and 93.1% and 82.9% for African-Americans. One- and 4-year patient survival rates for cadaver donor kidneys were 91.4% and 78.7% for non-African-Americans and 92.4% and 80.2% for African-Americans. One- and 5-year graft survival rates for cadaver kidneys were 84.6% and 73.7% for non-African-Americans and 84.6% and 68.9% for African-Americans. One- and 5-year graft and patient survival rates were identical for recipients of hepatitis C virus-positive and anti-HBc positive donors, with the exception of a trend to late graft loss in the African-American hepatitis C virus group due to higher rates of noncompliance, an effect that disappears with censoring of graft loss from that cause. The cadaveric renal transplant median waiting time for non-African-Americans was 391 days compared to 734 days nationally; the waiting time for African-Americans was 647 days compared to 1,335 days nationally. When looking at all patients, living and cadaver donor, the median waiting times are 220 days for non-African-Americans and 462 days for African-Americans. CONCLUSIONS Programs specifically oriented to improve volunteerism in African-Americans have led to a marked improvement in overall waiting time and in rates of living donation in this patient group. The median waiting times to cadaveric renal transplantation were also significantly shorter in the authors' center, especially for African-American patients, by taking advantage of the higher rates of hepatitis C infection and encouraging hepatitis B vaccination. These policies can markedly improve end-stage renal disease care for African-Americans by halving the overall waiting time while still achieving comparable graft and patient survival rates.
Figures
Similar articles
-
The UNOS Scientific Renal Transplant Registry.Clin Transpl. 1996:1-14. Clin Transpl. 1996. PMID: 9286555
-
The UNOS Scientific Renal Transplant Registry.Clin Transpl. 1998:1-16. Clin Transpl. 1998. PMID: 10503082
-
The UNOS Scientific Renal Transplant Registry--2000.Clin Transpl. 2000:1-18. Clin Transpl. 2000. PMID: 11512303
-
The UNOS Renal Transplant Registry: Review of the Last Decade.Clin Transpl. 2014:1-12. Clin Transpl. 2014. PMID: 26281122 Review.
-
Transplanting kidneys from donors with prior hepatitis B infection: one response to the organ shortage.J Nephrol. 2002 Nov-Dec;15(6):605-13. J Nephrol. 2002. PMID: 12495272 Review.
Cited by
-
Addressing racial and ethnic disparities in live donor kidney transplantation: priorities for research and intervention.Semin Nephrol. 2010 Jan;30(1):90-8. doi: 10.1016/j.semnephrol.2009.10.010. Semin Nephrol. 2010. PMID: 20116653 Free PMC article. Review.
-
Similar outcomes among black and white renal allograft recipients.J Am Soc Nephrol. 2009 Jan;20(1):172-9. doi: 10.1681/ASN.2007070820. Epub 2008 Oct 29. J Am Soc Nephrol. 2009. PMID: 18971374 Free PMC article.
-
Racial and Ethnic Disparities in Graft and Recipient Survival in Elderly Kidney Transplant Recipients.J Am Geriatr Soc. 2015 Dec;63(12):2485-2493. doi: 10.1111/jgs.13845. Epub 2015 Dec 11. J Am Geriatr Soc. 2015. PMID: 26660200 Free PMC article.
-
Patient attitudes toward mobile phone-based health monitoring: questionnaire study among kidney transplant recipients.J Med Internet Res. 2013 Jan 8;15(1):e6. doi: 10.2196/jmir.2284. J Med Internet Res. 2013. PMID: 23305649 Free PMC article.
-
Waiting-List and early posttransplant prognosis among ethnoracial groups: Data from the organ procurement and transplantation network.Front Surg. 2023 Jan 30;10:1045363. doi: 10.3389/fsurg.2023.1045363. eCollection 2023. Front Surg. 2023. PMID: 36793312 Free PMC article.
References
-
- Rettig RA, Levinsky NG, eds. Kidney failure and the federal government. Washington, DC: National Academy Press, 1991. - PubMed
-
- Brown JG. Inspector General. Racial and geographic disparity in the distribution of organs for transplantation. Department of Health and Human Services, Office of the Inspector General, June 1998;OEI-01-98-00360.
-
- Wolfe RA, Ashby BA, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999; 341: 1725–1730. - PubMed
-
- Ojo AO, Hanson JA, Meier-Kriesche H-U, et al. Survival in recipients of marginal cadaveric donor kidneys compared with other recipients and wait-listed transplant candidates. J Am Soc Nephrol 2001; 12: 589–597. - PubMed
-
- Schweitzer EJ, Wiland A, Evans D, et al. The shrinking renal replacement therapy “break-even” point. Transplantation 1998; 66: 1702–1708. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
