

Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate
- PMID: 12457349
- PMCID: PMC1986797
- DOI: 10.1053/jhsu.2002.35878
Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate
Abstract
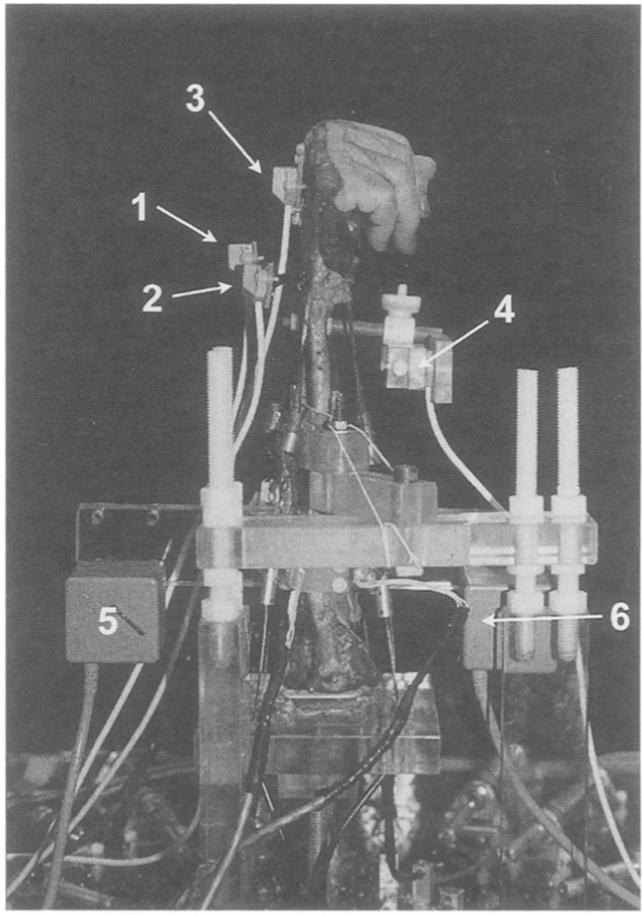
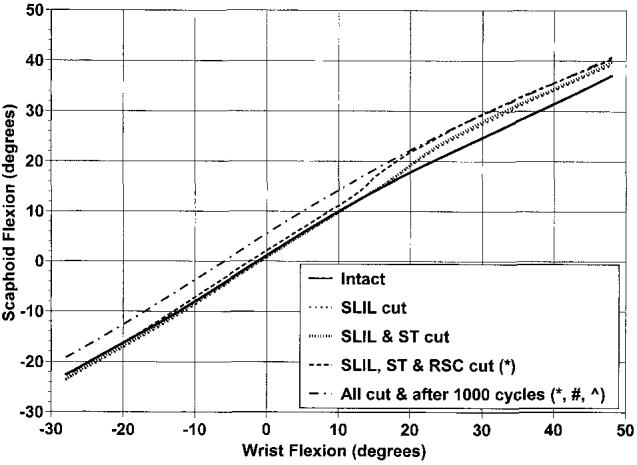
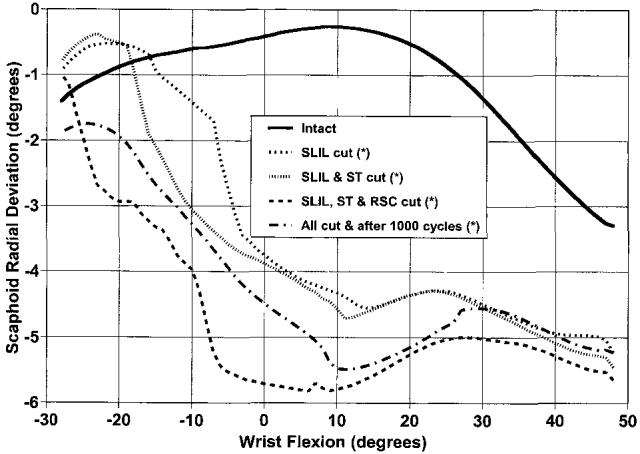
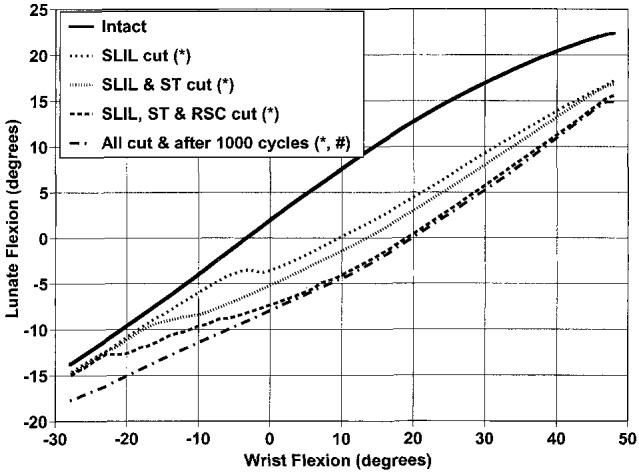
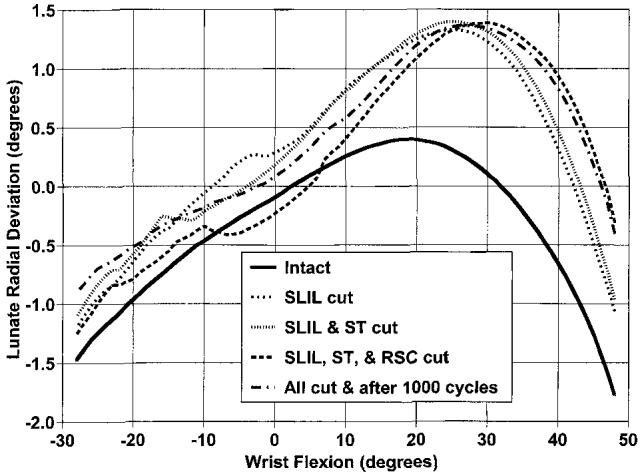
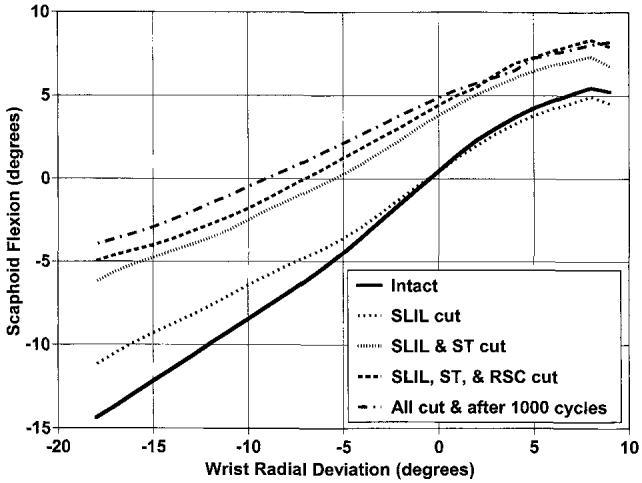
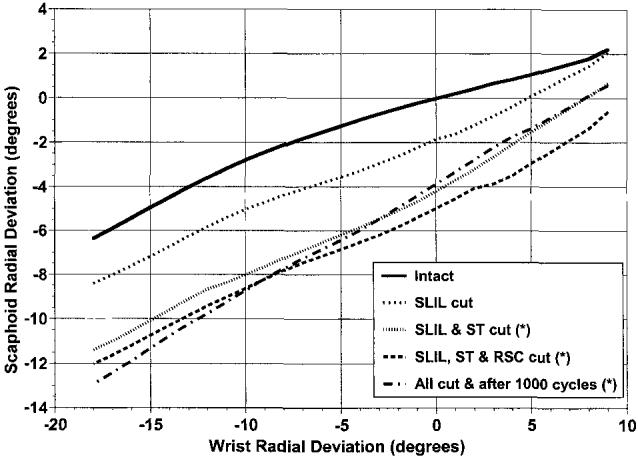
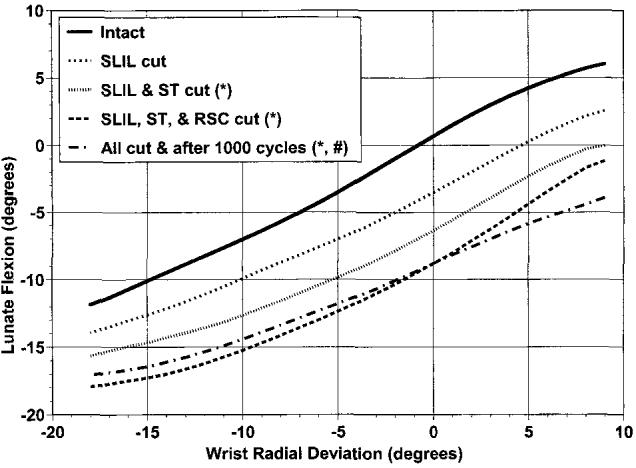
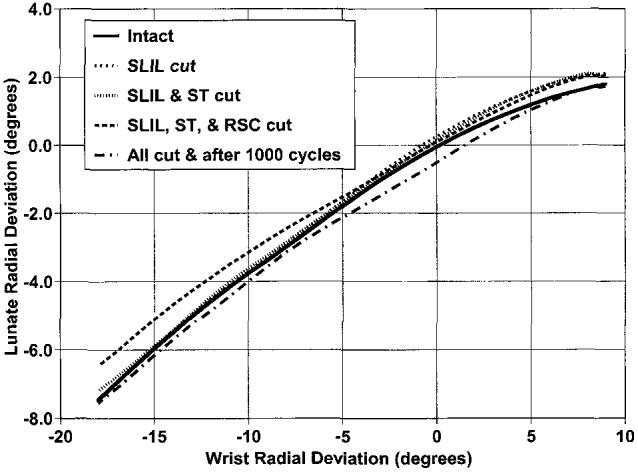
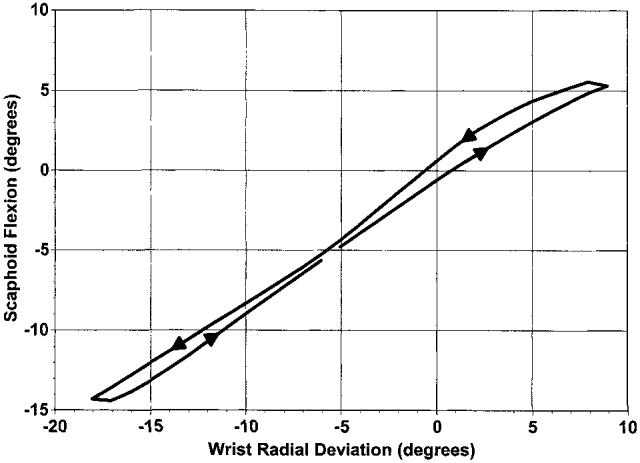
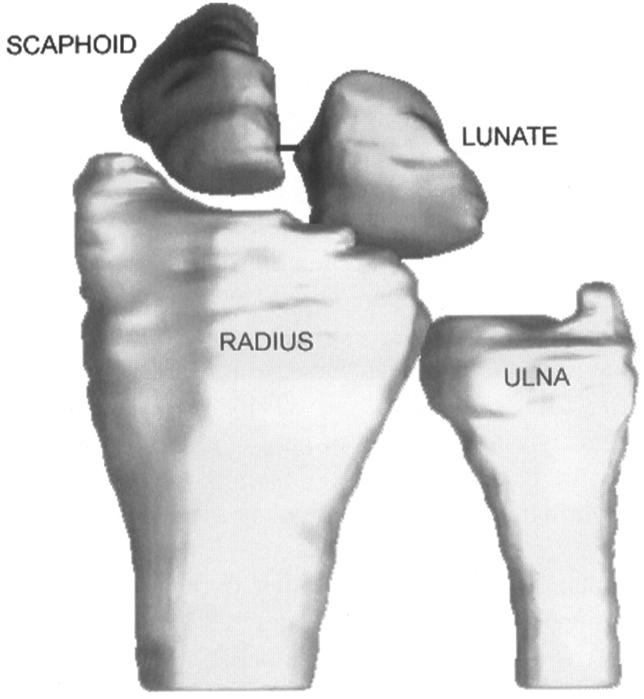
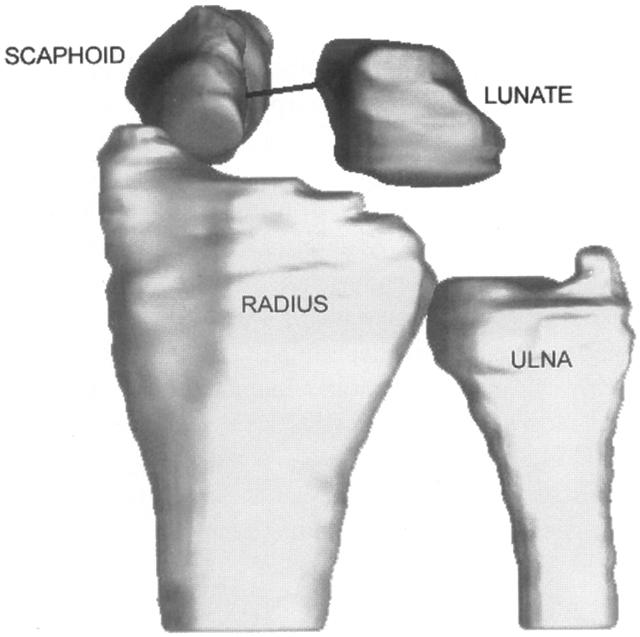
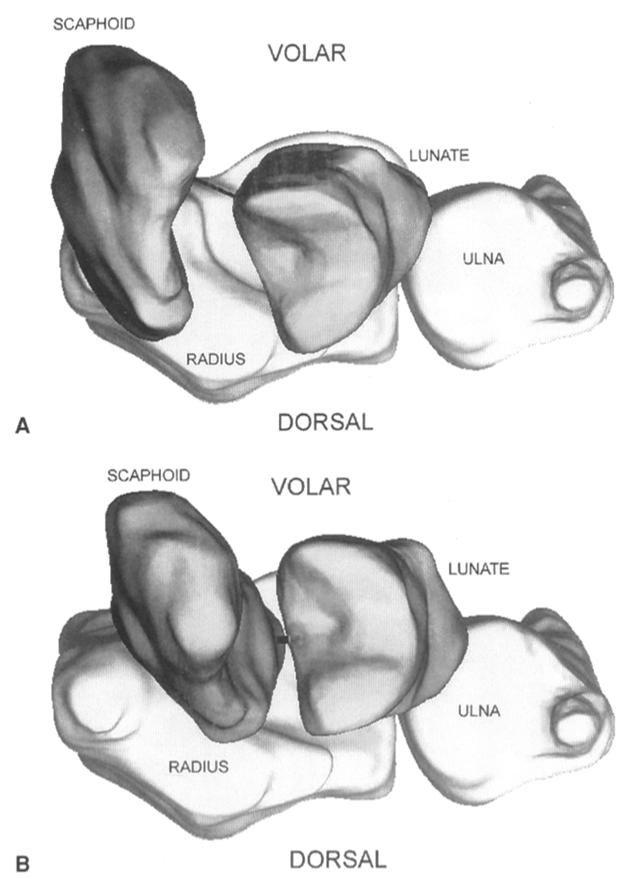
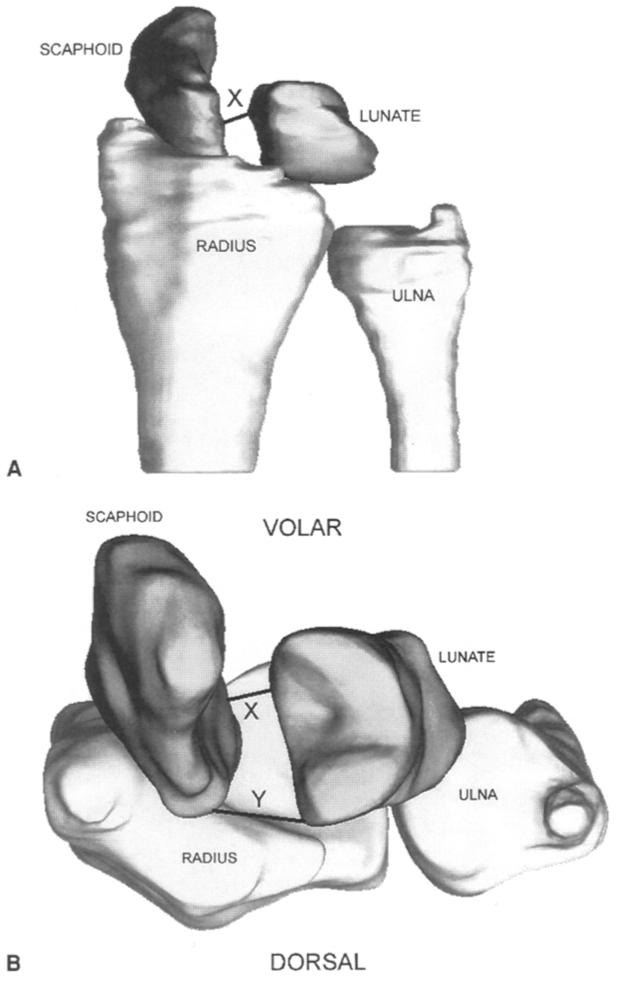
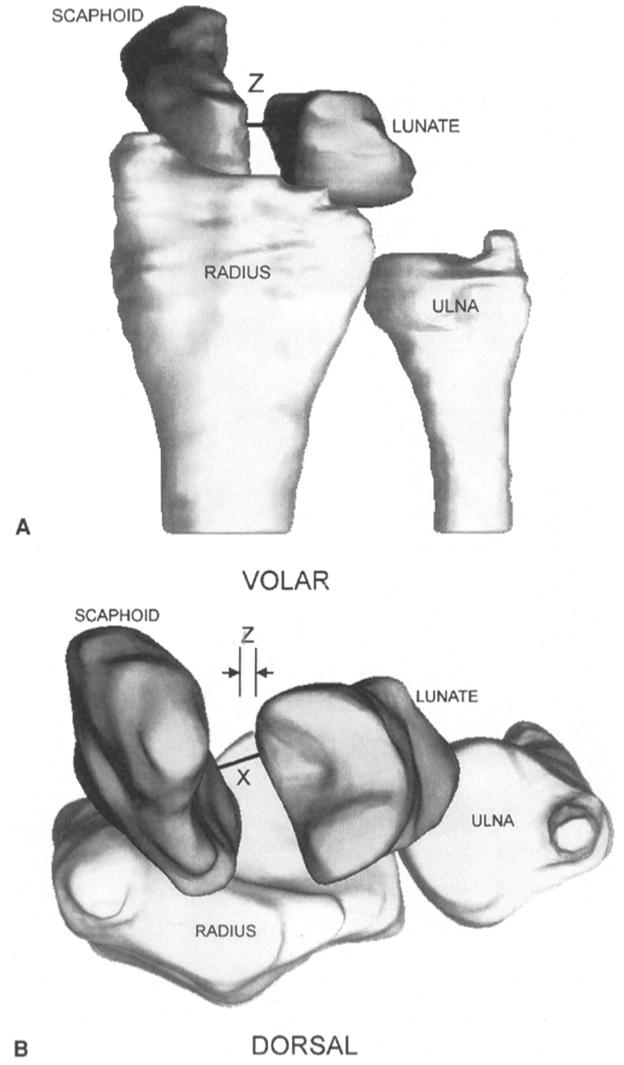
This study evaluated the effects of sectioning the scapholunate interosseous ligament, radioscaphocapitate ligament, and scaphotrapezial ligament on the kinematics of the scaphoid and lunate. Eight cadaver upper extremities were placed in a wrist joint simulator and moved in continuous cycles of flexion-extension and radial-ulnar deviation. Positional data of the scaphoid and lunate were obtained in the intact state, after the scapholunate ligament was cut; after the scapholunate and scaphotrapezial ligaments were cut; after the scapholunate, scaphotrapezial, and radioscaphocapitate ligaments were cut; and after all 3 ligaments were cut and the specimen was placed through an additional 1,000 cycles of flexion-extension. Cutting the scapholunate ligament caused changes in scaphoid and lunate motion during flexion-extension, but not radial-ulnar deviation. Additional sectioning of the scaphotrapezial ligament followed by the radioscaphocapitate ligament caused further kinematic changes in these carpal bones. One thousand cycles of motion after all 3 ligaments were sectioned caused additional kinematic changes in the scaphoid and lunate. The scapholunate ligament appears to be the primary stabilizer between the scaphoid and lunate. The radioscaphocapitate and scaphotrapezial ligaments are secondary restraints. Repetitive cyclic motion after ligament sectioning appears to have additional deleterious effects on carpal kinematics.
Figures
References
-
- Berger RA. The gross and histologic anatomy of the scapholunate interosseous ligament. J Hand Surg. 1996;21A:170–178. - PubMed
-
- Berger RA, Landsmeer JMF. The palmar radiocarpal ligaments: a study of adult and fetal human wrist joints. J Hand Surg. 1990;15A:847–854. - PubMed
-
- Berger RA. The ligaments of the wrist. A current overview of anatomy with considerations of their potential functions. Hand Clin. 1997;13:63–82. - PubMed
-
- Moritomo H, Viegas SF, Nakamura K, DaSilva MF, Patterson RM. The scaphotrapezio-trapezoidal joint. Part 1: an anatomic and radiographic study. J Hand Surg. 2000;25A:899–910. - PubMed
-
- Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg. 1985;10A:492–498. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
