

Critical role for CXCR2 and CXCR2 ligands during the pathogenesis of ventilator-induced lung injury
- PMID: 12464676
- PMCID: PMC151632
- DOI: 10.1172/JCI15849
Critical role for CXCR2 and CXCR2 ligands during the pathogenesis of ventilator-induced lung injury
Abstract
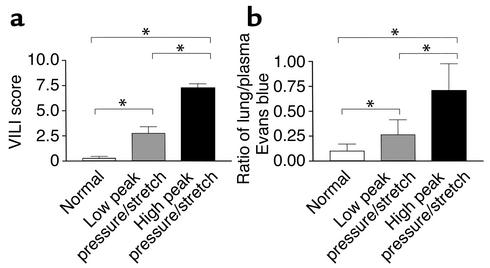
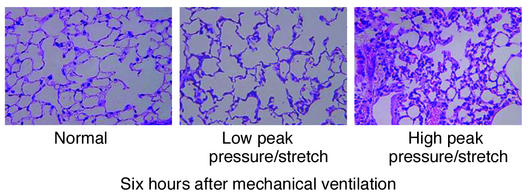
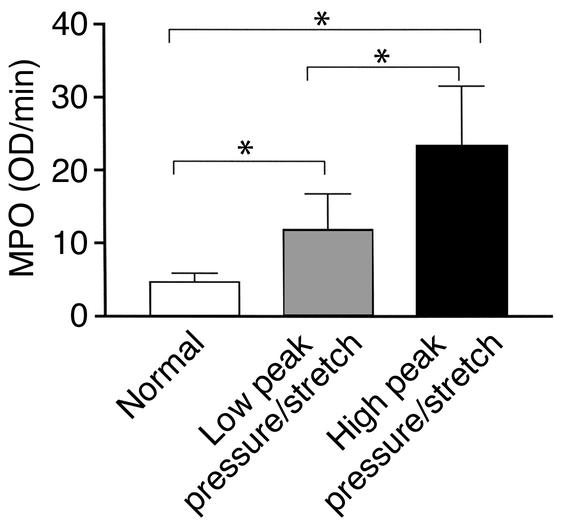
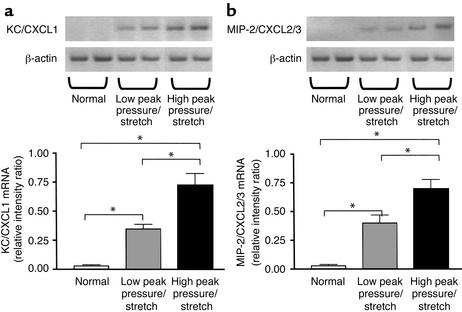
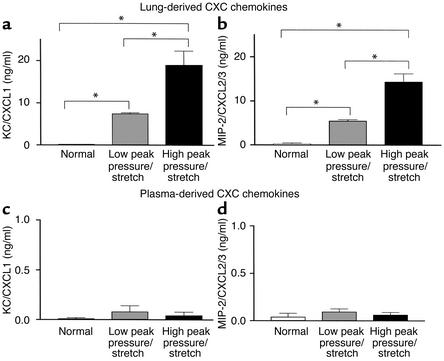
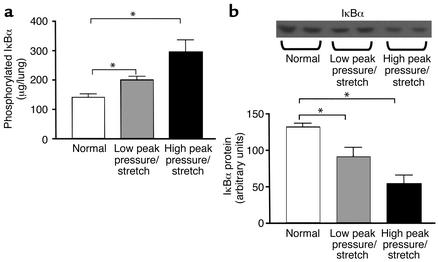
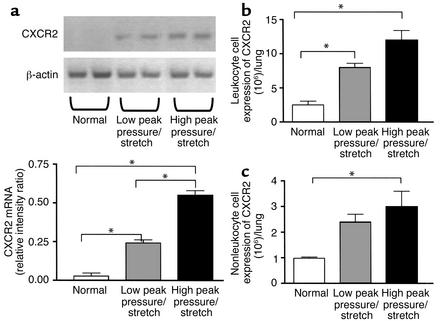
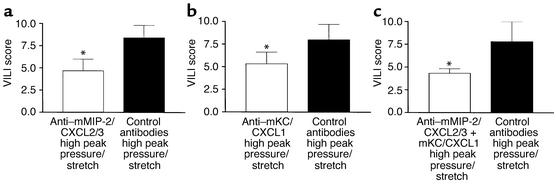
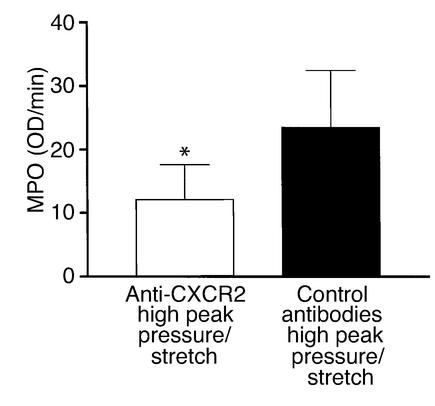
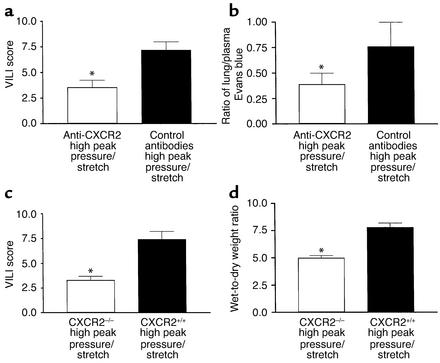
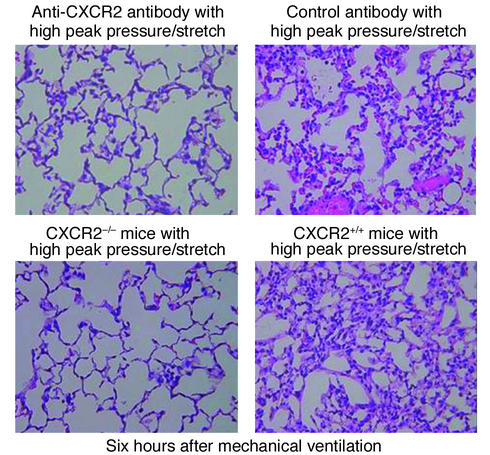
Mortality related to adult respiratory distress syndrome (ARDS) ranges from 35% to 65%. Lung-protective ventilator strategies can reduce mortality during ARDS. The protective strategies limit tidal volumes and peak pressures while maximizing positive end-expiratory pressure. The efficacy of this approach is due to a reduction of shear-stress of the lung and release of inflammatory mediators. Ventilator-induced lung injury (VILI) is characterized by inflammation. The specific mechanism(s) that recruit leukocytes during VILI have not been elucidated. Because the murine CXC chemokines KC/CXCL1 and MIP-2/CXCL2/3, via CXCR2, are potent neutrophil chemoattractants, we investigated their role in a murine model of VILI. We compared two ventilator strategies in C57BL/6 mice: high peak pressure and high stretch (high peak pressure/stretch) versus low peak pressure/stretch for 6 hours. Lung injury and neutrophil sequestration from the high-peak pressure/stretch group were greater than those from the low-peak pressure/stretch group. In addition, lung expression of KC/CXCL1 and MIP-2/CXCL2/3 paralleled lung injury and neutrophil sequestration. Moreover, in vivo inhibition of CXCR2/CXC chemokine ligand interactions led to a marked reduction in neutrophil sequestration and lung injury. These findings were confirmed using CXCR2(-/-) mice. Together these experiments support the notion that increased expression of KC/CXCL1 and MIP-2/CXCL2/3 and their interaction with CXCR2 are important in the pathogeneses of VILI.
Figures
Comment in
-
Neutrophils and lung injury: getting it right.J Clin Invest. 2002 Dec;110(11):1603-5. doi: 10.1172/JCI17302. J Clin Invest. 2002. PMID: 12464663 Free PMC article. No abstract available.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Ranieri VM, et al. Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1999;282:54–61. - PubMed
-
- Kollef MH, Schuster DP. The acute respiratory distress syndrome. N Engl J Med. 1995;332:27–37. - PubMed
-
- Dreyfuss D, Soler P, Basset G, Saumon G. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis. 1988;137:1159–1164. - PubMed
-
- Corbridge TC, et al. Adverse effects of large tidal volume and low PEEP in canine acid aspiration. Am Rev Respir Dis. 1990;142:311–315. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
