

Association between bacterial vaginosis or chlamydial infection and miscarriage before 16 weeks' gestation: prospective community based cohort study
- PMID: 12468483
- PMCID: PMC137811
- DOI: 10.1136/bmj.325.7376.1334
Association between bacterial vaginosis or chlamydial infection and miscarriage before 16 weeks' gestation: prospective community based cohort study
Abstract
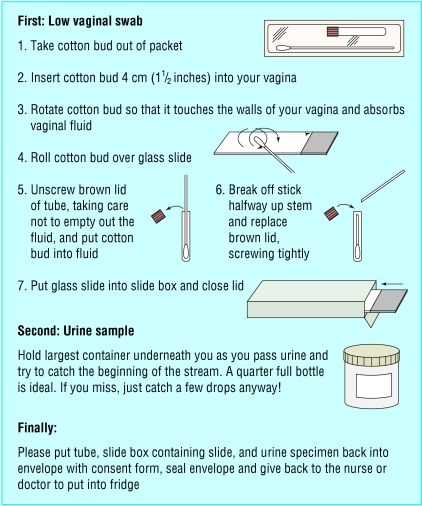
Objectives: To assess whether bacterial vaginosis or chlamydial infection before 10 weeks' gestation is associated with miscarriage before 16 weeks.
Design: Prospective cohort study.
Setting: 32 general practices and five family planning clinics in south London.
Participants: 1216 pregnant women, mean age 31, presenting before 10 weeks' gestation.
Main outcome measure: Prevalence of miscarriage before 16 weeks' gestation.
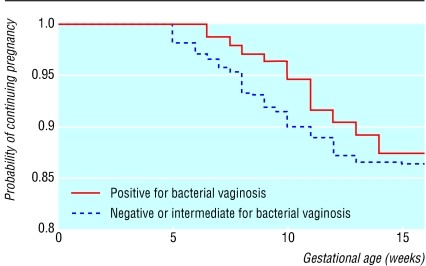
Results: 121 of 1214 women (10.0%, 95% confidence interval 8.3% to 11.7%) miscarried before 16 weeks. 174 of 1201 women (14.5%, 12.5% to 16.5%) had bacterial vaginosis. Compared with women who were negative for bacterial vaginosis those who were positive had a relative risk of miscarriage before 16 weeks' gestation of 1.2 (0.7 to 1.9). Bacterial vaginosis was, however, associated with miscarriage in the second trimester at 13-15 weeks (3.5, 1.2 to 10.3). Only 29 women (2.4%, 1.5% to 3.3%) had chlamydial infection, of whom one miscarried (0.32, 0.04 to 2.30).
Conclusion: Bacterial vaginosis is not strongly predictive of early miscarriage but may be a predictor after 13 weeks' gestation. The prevalence of Chlamydia was too low to assess the risk, but it is unlikely to be a major risk factor in pregnant women.
Figures
References
-
- McGregor J, French J, Parker R, Draper D, Patterson E, Jones W, et al. Prevention of premature birth by screening and treatment for common genital tract infections: results of a prospective controlled evaluation. Am J Obstet Gynecol. 1995;173:157–167. - PubMed
-
- Eschenbach DA. Chlamydia trachomatis in pregnancy. In: Bowie WR, Caldwell HD, Jones RP, Mardh P-A, Ridgway GL, Schachter J, editors. Chlamydial infections. Cambridge: Cambridge University Press; 1990. pp. 329–339.
-
- Morgan DJ, Aboud CJ, McCaffrey MB, Bhide SA, Lamont RF, Taylor-Robinson D. Comparison of Gram-stained smears prepared from blind vaginal swabs with those obtained at speculum examination for the assessment of vaginal flora. Br J Obstet Gynaecol. 1996;103:1105–1108. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical