

Biopsy surveillance is still necessary in patients with Barrett's oesophagus despite new endoscopic imaging techniques
- PMID: 12477753
- PMCID: PMC1773515
- DOI: 10.1136/gut.52.1.18
Biopsy surveillance is still necessary in patients with Barrett's oesophagus despite new endoscopic imaging techniques
Abstract
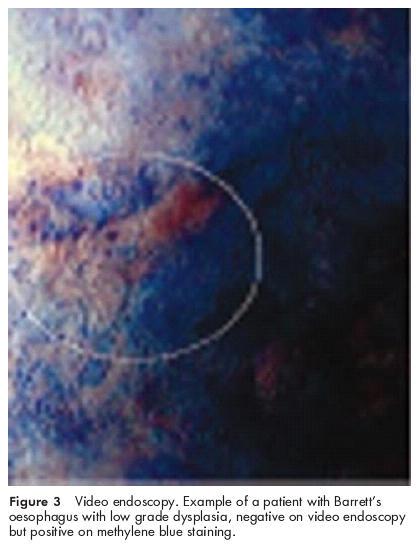
Background and aims: Endoscopic surveillance including stepwise four quadrant biopsies (4QB) is still regarded as the standard approach in patients with Barrett's oesophagus (BO). Several methods such as dye staining with methylene blue (MB) and tissue autofluorescence (AF) have been advocated to reduce the number of biopsies. We assessed their sensitivity and specificity compared with the standard approach-that is, endoscopy with 4QB-in the surveillance of a mixed BO population.
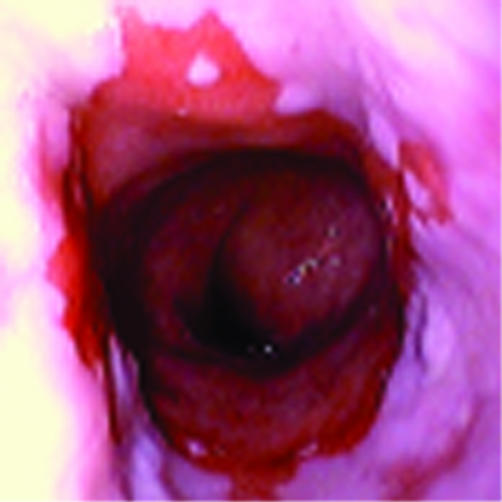
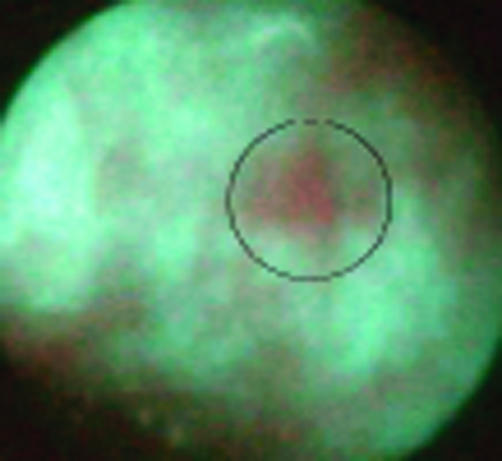
Patients and methods: Thirty five consecutive BO patients (mean age 64.9 years; 30 men, five women) were included in the study. AF endoscopy was followed by high resolution video endoscopy (VE) plus tissue staining with 0.5% MB. Biopsies were taken from any suspicious area found on any of the above tests, in addition to 4QB every 2 cm. The results were classified as either positive or negative for the various tests used. Histopathological results were used as the reference standard.
Results: In the 35 study patients, a total of 345 biopsies showed low grade dysplasia (LGD) in 88 biopsies, high grade dysplasia (HGD) in 19 biopsies, and carcinoma in 12 biopsies. The sensitivity and specificity rates for AF and MB for the diagnosis of cancer or dysplasia versus BO mucosa without dysplasia were 21%/91% and 37%/91%, respectively. 4QB revealed five cancer/HGD areas and 76 LGD areas not detected by AF, MB, or VE. The additional yield of MB and AF over VE with 4QB concerned only one HGD area (in the vicinity of a cancer) and seven LGD areas.
Conclusions: Due to their low sensitivity, AF and MB are not suitable techniques for reducing the high numbers of routine biopsies needed for finding additional foci of HGD or cancer. Careful endoscopic observation and stepwise four quadrant biopsy therefore still represent the gold standard for surveillance of Barrett's oesophagus.
Figures
Comment in
-
New imaging techniques: promise or passe.Gut. 2003 Jul;52(7):1072. doi: 10.1136/gut.52.7.1072. Gut. 2003. PMID: 12801975 Free PMC article. No abstract available.
-
[Diagnosis and surveillance in patients with Barrett's esophagus].Z Gastroenterol. 2003 Sep;41(9):939-42. doi: 10.1055/s-2003-41828. Z Gastroenterol. 2003. PMID: 13130333 German. No abstract available.
Comment on
-
S, m, l, xl.Gut. 2003 Jan;52(1):5-7. doi: 10.1136/gut.52.1.5. Gut. 2003. PMID: 12477746 Free PMC article. No abstract available.
References
-
- Hameeteman W, Tytgat GNJ, Houthoff HJ, et al. Barrett’s esophagus: development of dysplasia and adenocarcinoma. Gastroenterology 1989;96:1249–56. - PubMed
-
- Drewitz DJ, Sampliner RE, Garewal HS. Long term follow-up of Barrett’s cohort. Am J Gastroenterol 1997;92:212–15. - PubMed
-
- Dent J, Bremner CD, Collen MJ, et al. Working party report to the World Congress of Gastroenterology, Sydney, 1990: Barrett’s esophagus. J Gastroenterol Hepatol 1991;6:1–22. - PubMed
-
- Cameron AJ, Ott BJ, Payne WS. The incidence of adenocarcinoma in columnar-lined (Barrett’s) esophagus. N Engl J Med 1985;313:857–9. - PubMed
-
- Spechler SJ, Robbins AH, Rubins HB, et al. Adenocarcinoma and Barrett’s esophagus: an overrated risk? Gastroenterology 1984;87:927–33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous