

High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS duration
- PMID: 12482792
- PMCID: PMC1767510
- DOI: 10.1136/heart.89.1.54
High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS duration
Abstract
Objective: To study the possible occurrence of left ventricular (LV) systolic and diastolic asynchrony in patients with systolic heart failure (HF) and narrow QRS complexes.
Design: Prospective study.
Setting: University teaching hospital.
Patients: 200 subjects were studied by echocardiography. 67 patients had HF and narrow QRS complexes (< or = 120 ms), 45 patients had HF and wide QRS complexes (> 120 ms), and 88 served as normal controls.
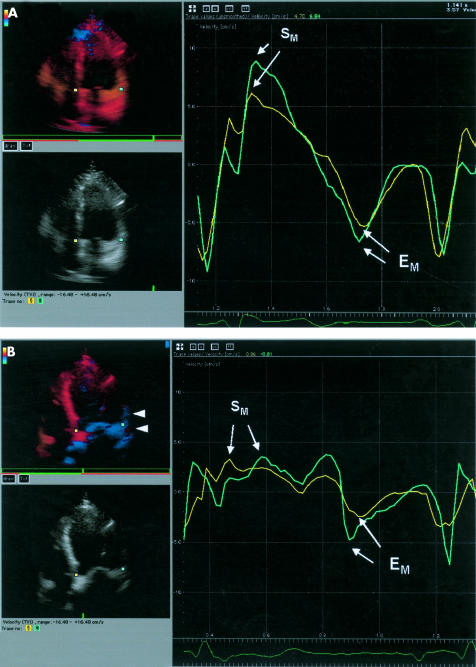
Interventions: Echocardiography with tissue Doppler imaging was performed using a six basal, six mid-segmental model.
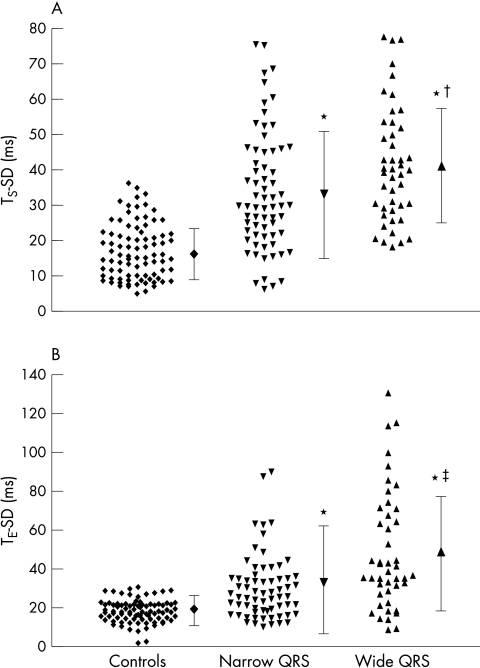
Main outcome measures: Severity and prevalence of systolic and diastolic asynchrony, as assessed by the maximal difference in time to peak myocardial systolic contraction (T(S)) and early diastolic relaxation (T(E)), and the standard deviation of T(S) (T(S)-SD) and of T(E) (T(E)-SD) of the 12 LV segments.
Results: The mean (SD) maximal difference in T(S) (controls 53 (23) ms v narrow QRS 107 (54) ms v wide QRS 130 (51) ms, both p < 0.001 v controls) and in T(S)-SD (controls 17.0 (7.8) ms v narrow QRS 33.8 (16.9) ms v wide QRS 42.0 (16.5) ms, both p < 0.001 v controls) was prolonged in the narrow QRS group compared with normal controls. Similarly, the maximal difference in T(E) (controls 59 (19) ms v narrow QRS 104 (71) ms v wide QRS 148 (87) ms, both p < 0.001 v controls) and in T(E)-SD (controls 18.5 (5.8) ms v narrow QRS 33.3 (27.7) ms v wide QRS 48.6 (30.2) ms, both p < 0.001 v controls) was prolonged in the narrow QRS group. The prevalence of systolic and diastolic asynchrony was 51% and 46%, respectively, in the narrow QRS group, and 73% and 69%, respectively, in the wide QRS group. Stepwise multiple regression analysis showed that a low mean myocardial systolic velocity from the six basal LV segments and a large LV end systolic diameter were independent predictors of systolic asynchrony, while a low mean myocardial early diastolic velocity and QRS complex duration were independent predictors of diastolic asynchrony.
Conclusions: LV systolic and diastolic mechanical asynchrony is common in patients with HF with narrow QRS complexes. As QRS complex duration is not a determinant of systolic asynchrony, it implies that assessment of intraventricular synchronicity is probably more important than QRS duration in considering cardiac resynchronisation treatment.
Figures
References
-
- Cazeau S, Leclercq C, Lavergne T, et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med 2001;344:873–80. - PubMed
-
- Gras D, Mabo P, Tang T, et al. Multisite pacing as a supplemental treatment of congestive heart failure: preliminary results of the Medtronic Inc. InSync study. Pacing Clin Electrophysiol 1998;21:2249–55. - PubMed
-
- Kass DA, Chen CH, Curry C, et al. Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circulation 1999;99:1567–73. - PubMed
-
- Nelson GS, Curry CW, Wyman BT, et al. Predictors of systolic augmentation from left ventricular preexcitation in patients with dilated cardiomyopathy and intraventricular conduction delay. Circulation 2000;101:2703–9. - PubMed
-
- Morris-Thurgood JA, Turner MS, Nightingale AK, et al. Pacing in heart failure: improved ventricular interaction in diastole rather than systolic re-synchronization. Europace 2000;2:271–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous