

Catecholaminergic polymorphic ventricular tachycardia: electrocardiographic characteristics and optimal therapeutic strategies to prevent sudden death
- PMID: 12482795
- PMCID: PMC1767500
- DOI: 10.1136/heart.89.1.66
Catecholaminergic polymorphic ventricular tachycardia: electrocardiographic characteristics and optimal therapeutic strategies to prevent sudden death
Abstract
Objective: To investigate the clinical outcome, ECG characteristics, and optimal treatment of catecholaminergic polymorphic ventricular tachycardia (CPVT), a malignant and rare ventricular tachycardia.
Patients and methods: Questionnaire responses and ECGs of 29 patients with CPVT were evaluated. Mean (SD) age of onset was 10.3 (6.1) years.
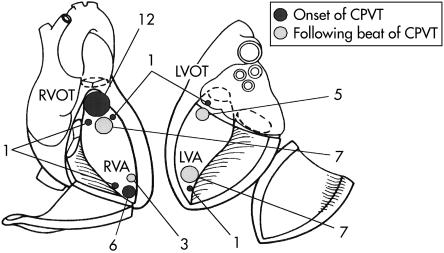
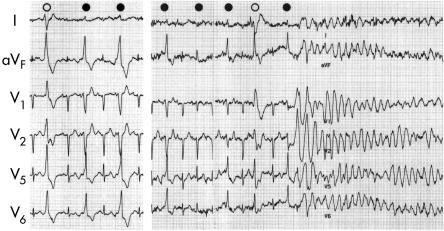
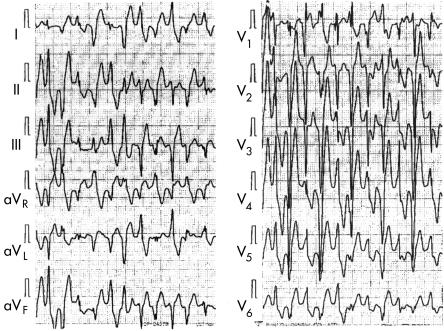
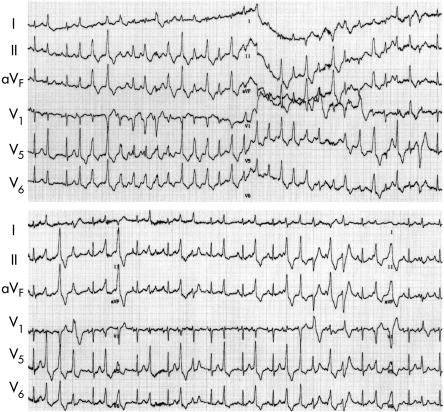
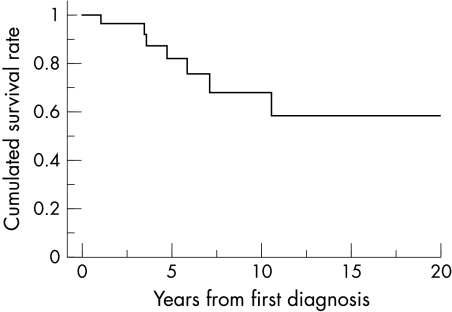
Results: The initial CPVT manifestations were syncope (79%), cardiac arrest (7%), and a family history (14%). ECGs showed sinus bradycardia and a normal QTc. Mean heart rate during CPVT was 192 (30) beats/min. Most cases were non-sustained (72%), but 21% were sustained and 7% were associated with ventricular fibrillation. The morphology of CPVT was polymorphic (62%), polymorphic and bidirectional (21%), bidirectional (10%), or polymorphic with ventricular fibrillation (7%). There was 100% inducement of CPVT by exercise, 75% by catecholamine infusion, and none by programmed stimulation. No late potential was recorded. Onset was in the right ventricular outflow tract in more than half the cases. During a follow up of 6.8 (4.9) years, sudden death occurred in 24% of the patients, 7% of whom had anoxic brain damage. Autosomal dominant inheritance was seen in 8% of the patients' families. beta Blockers completely controlled CPVT in only 31% of cases. Calcium antagonists partially suppressed CPVT in autosomal dominant cases.
Conclusions: CPVT may arise in certain distinct areas but the prognosis is poor. The onset of CPVT may be an indication for an implanted cardioverter-defibrillator.
Figures
References
-
- Berg KJ. Multifocal ventricular extrasystoles with Adams-Stokes syndrome in siblings. Am Heart J 1960;60:966–70.
-
- Wennewold A, Melchior JC, Sandoe E. Adams-Stokes syndrome in children without organic heat disease: electrocardiogram after exercise as a diagnostic tool. Acta Med Scand 1965;177:557–63. - PubMed
-
- Dik T, Janukowicz C. Bidirectional tachycardia in a case of recurrent paroxysmal tachycardia with ventricular fibrillation. Cardiologia 1968;52:132–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources