

Mechanism of lumen enlargement with direct stenting versus predilatation stenting: influence of remodelling and plaque characteristics assessed by volumetric intracoronary ultrasound
- PMID: 12482801
- PMCID: PMC1767502
- DOI: 10.1136/heart.89.1.84
Mechanism of lumen enlargement with direct stenting versus predilatation stenting: influence of remodelling and plaque characteristics assessed by volumetric intracoronary ultrasound
Abstract
Objective: To compare the effects of arterial remodelling and plaque characteristics on the mechanisms of direct stenting and predilatation stenting. Direct stenting has become routine in some laboratories and differs technically from predilatation stenting.
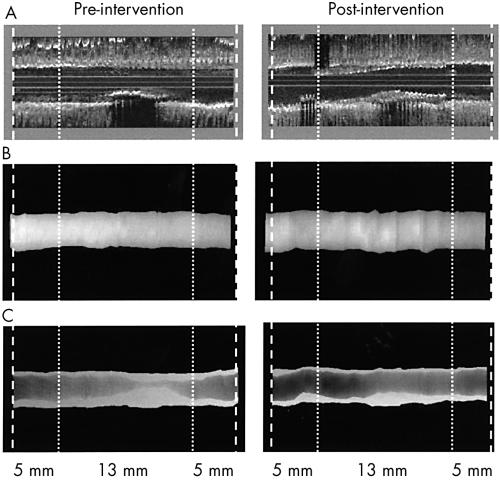
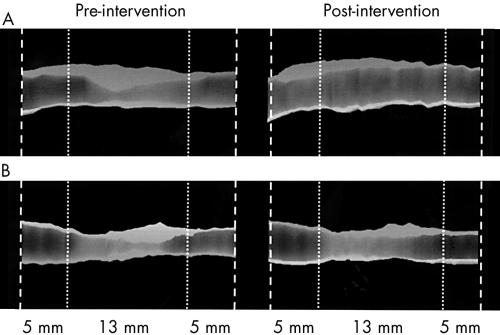
Methods: Pre- and post-interventional volumetric intravascular ultrasound (IVUS) was undertaken in 30 patients with direct stenting and in 30 with predilatation stenting of non-calcified native coronary lesions, using the same stent design and stent length. Lumen, vessel (external elastic membrane (EEM)), and plaque (plaque + media) volumes were calculated. Remodelling was determined by comparing the EEM area at the centre of the lesion with the EEM areas at proximal and distal reference sites. Plaque eccentricity was defined as the thinnest plaque diameter to the thickest plaque diameter ratio. Plaque composition was characterised as soft, mixed, or dense.
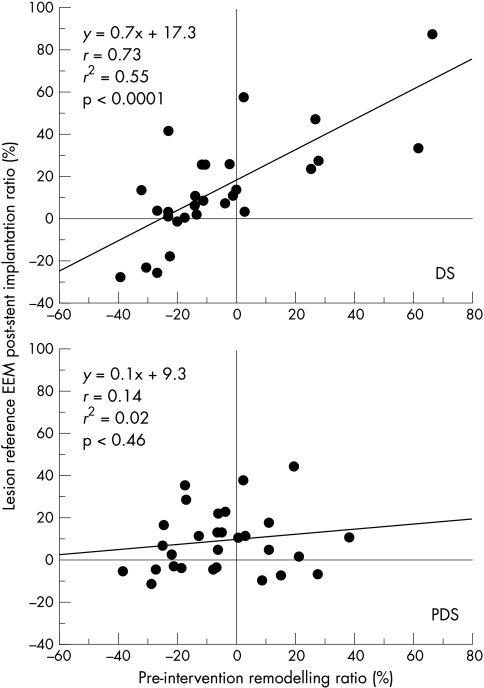
Results: All volumetric IVUS changes were similar in the two groups. Pre-intervention remodelling remained uninfluenced after direct stenting, but was neutralised after predilatation stenting. Eccentric lesions responded to intervention by a greater luminal gain owing to greater vessel expansion in direct stenting. Plaque composition influenced luminal gain in direct stenting, the gain being greatest in the softest plaques; in predilatation stenting, luminal gain was equivalent but vessel expansion was greater for "dense" plaque and plaque reduction greater for "soft" plaque.
Conclusions: In non-calcified lesions, the mechanisms of lumen enlargement after direct or predilatation stenting are significantly influenced by atherosclerotic remodelling, plaque eccentricity, and plaque composition.
Figures
Similar articles
-
Comparative analysis of lumen enlargement mechanisms achieved with the bifurcation dedicated BiOSS) stent versus classical coronary stent implantations by means of provisional side branch stenting strategy: an intravascular ultrasound study.Int J Cardiovasc Imaging. 2013 Dec;29(8):1667-76. doi: 10.1007/s10554-013-0264-0. Epub 2013 Jul 19. Int J Cardiovasc Imaging. 2013. PMID: 23868287 Free PMC article. Clinical Trial.
-
Impact of kissing balloon inflation on the main vessel stent volume, area, and symmetry after side-branch dilation in patients with coronary bifurcation lesions: a serial volumetric intravascular ultrasound study.JACC Cardiovasc Interv. 2013 Sep;6(9):923-31. doi: 10.1016/j.jcin.2013.04.019. Epub 2013 Aug 14. JACC Cardiovasc Interv. 2013. PMID: 23954062
-
Effect of disease eccentricity on compensatory remodeling of coronary arteries: evidence from intravascular ultrasound before interventions.Int J Cardiol. 2002 Nov;86(1):99-105. doi: 10.1016/s0167-5273(02)00197-3. Int J Cardiol. 2002. PMID: 12243854
-
[New methods of coronary imaging II. Intracoronary ultrasonography in clinical practice].Ital Heart J Suppl. 2001 Jun;2(6):579-92. Ital Heart J Suppl. 2001. PMID: 11460831 Review. Italian.
-
[The form of atherosclerotic coronary plaques: pathoanatomic concepts and new insights using intravascular ultrasound].Z Kardiol. 1994 Oct;83(10):717-26. Z Kardiol. 1994. PMID: 7810185 Review. German.
Cited by
-
Three-dimensional visualization of scoring mechanism of 'AngioSculpt' balloon for calcified coronary lesions using optical coherence tomography.J Cardiol Cases. 2011 Nov 27;5(1):e16-e19. doi: 10.1016/j.jccase.2011.10.008. eCollection 2012 Feb. J Cardiol Cases. 2011. PMID: 30532893 Free PMC article.
-
Mechanical properties of normal and diseased cerebrovascular system.J Vasc Interv Neurol. 2009 Apr;2(2):155-62. J Vasc Interv Neurol. 2009. PMID: 22518247 Free PMC article.
-
Comparative analysis of lumen enlargement mechanisms achieved with the bifurcation dedicated BiOSS) stent versus classical coronary stent implantations by means of provisional side branch stenting strategy: an intravascular ultrasound study.Int J Cardiovasc Imaging. 2013 Dec;29(8):1667-76. doi: 10.1007/s10554-013-0264-0. Epub 2013 Jul 19. Int J Cardiovasc Imaging. 2013. PMID: 23868287 Free PMC article. Clinical Trial.
References
-
- Pasterkamp G, Borst C, Gussenhoven EJ, et al. Reremodeling of de novo atherosclerotic lesions in femoral arteries: impact on mechanism of balloon angioplasty. J Am Coll Cardiol 1995;26:422–8. - PubMed
-
- Honye J, Mahon DJ, Jain A, et al. Morphological effects of coronary balloon angioplasty in vivo assessed by intravascular ultrasound imaging. Circulation 1992;85:1012–25. - PubMed
-
- Timmis SBH, Burns WJ, Hermiller JB, et al. Influence of coronary atherosclerotic remodeling on the mechanism of balloon angioplasty. Am Heart J 1997;134:1099–106. - PubMed
-
- Pentousis D, Guerin Y, Funck F, et al. Direct stent implantation without predilation using the multilink stent. Am J Cardiol 1998;82:1437–40. - PubMed
-
- Ormiston JA, Webster MWI, Ruygrok PN, et al. A randomized study of direct coronary stent delivery with stenting after predilation: the NIR future trail. Cathet Cardiovasc Intervent 2000;50:377–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical