

Coronary artery anomalies--current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines
- PMID: 12484611
- PMCID: PMC140289
Coronary artery anomalies--current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines
Abstract
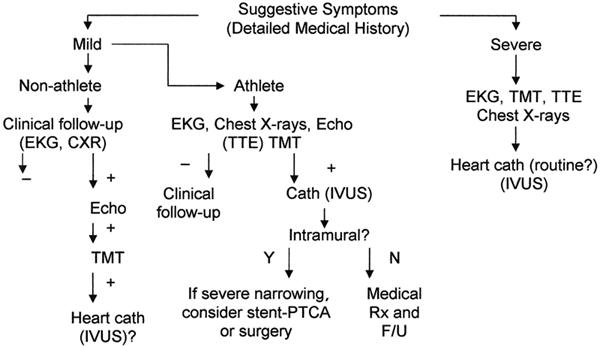
The study of coronary artery anomalies would benefit from the clarification of various fundamental issues, including the definitions, classification, incidence, pathophysiologic mechanisms, and clinical relevance of each anomaly. The greatest challenge is to identify the abnormality and determine its clinical relevance so that appropriate treatment can be instituted. Currently, the coronary anatomy is essentially defined by the features of the (conductive) epicardial coronary tree and its dependent territory. Therefore, one must consider all the possible and observed variations in anatomic features that are used to describe the coronary arteries. We propose that the left anterior descending, circumflex, and right coronary arteries be considered the essential elementary units of coronary anatomy. We also suggest that the coronary arteries be defined not by their origin or proximal course, but by their intermediate and distal segments or dependent microvascular bed. A strict classification system is necessary before meaningful data can be gathered about the incidence of coronary anomalies. With respect to clinical relevance, the greatest challenge is presented by anomalies that only occasionally cause critically severe clinical events and are otherwise compatible with a normal life. In such cases, it is not known whether the specific features of a given anomaly cause adverse clinical consequences, or whether additional episodic factors are required. To correlate subclassifiable anatomic and functional features with clinical events and prognoses, a large, multicenter database, relying on prospective, coordinated protocols, is urgently needed. In the absence of established official guidelines, we present practical protocols for diagnosing and treating coronary anomalies.
Figures
Similar articles
-
Anomalous origin of the right coronary artery from the left anterior descending artery: review of the literature.Cardiol J. 2012;19(2):122-9. Cardiol J. 2012. PMID: 22461044 Review.
-
Normal and anomalous coronary arteries: definitions and classification.Am Heart J. 1989 Feb;117(2):418-34. doi: 10.1016/0002-8703(89)90789-8. Am Heart J. 1989. PMID: 2644796 Review.
-
[Angina due to anatomical anomalies and to functional changes in the epicardial coronary vessels].Cardiologia. 1991 Dec;36(12 Suppl 1):149-59. Cardiologia. 1991. PMID: 1841764 Italian.
-
Single right coronary artery continuing as left circumflex artery and hypoplastic left anterior descending artery: a rare coronary anomaly.J Invasive Cardiol. 2008 Jun;20(6):E192-4. J Invasive Cardiol. 2008. PMID: 18523335
-
Incidence and clinical relevance of primary congenital anomalies of the coronary arteries in children and adults.Cardiol Young. 2013 Jun;23(3):381-6. doi: 10.1017/S1047951112000959. Epub 2012 Jul 20. Cardiol Young. 2013. PMID: 22813715
Cited by
-
Single coronary artery with anomalous origin from the right sinus Valsalva.Clin Res Cardiol. 2006 Feb;95(2):119-21. doi: 10.1007/s00392-006-0330-x. Epub 2006 Jan 16. Clin Res Cardiol. 2006. PMID: 16598522
-
Acute coronary syndrome on non-electrocardiogram-gated contrast-enhanced computed tomography.World J Radiol. 2022 Feb 28;14(2):30-46. doi: 10.4329/wjr.v14.i2.30. World J Radiol. 2022. PMID: 35317242 Free PMC article. Review.
-
Percutaneous coronary intervention for congenital absence of the right coronary artery with acute myocardial infarction: A case report and literature review.Medicine (Baltimore). 2020 Jan;99(5):e18981. doi: 10.1097/MD.0000000000018981. Medicine (Baltimore). 2020. PMID: 32000431 Free PMC article. Review.
-
Unilateral and multilateral congenital coronary-pulmonary fistulas in adults: clinical presentation, diagnostic modalities, and management with a brief review of the literature.Clin Cardiol. 2014 Sep;37(9):536-45. doi: 10.1002/clc.22297. Epub 2014 Sep 5. Clin Cardiol. 2014. PMID: 25196980 Free PMC article. Review.
-
Treatment of Anomalous Coronary Arteries-Surgical Revascularisation Using the Pure Internal Thoracic Artery Technique.J Cardiovasc Dev Dis. 2023 Apr 2;10(4):155. doi: 10.3390/jcdd10040155. J Cardiovasc Dev Dis. 2023. PMID: 37103034 Free PMC article.
References
-
- Angelini P, Villason S, Chan AV Jr, Diez JG. Normal and anomalous coronary arteries in humans. In: Angelini P, editor. Coronary artery anomalies: a comprehensive approach. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 27–150.
-
- Angelini P, de la Cruz MV, Valencia AM, Sanchez-Gomez C, Kearney DL, Sadowinski S, Real GR. Coronary arteries in transposition of the great arteries. Am J Cardiol 1994;74:1037–41. - PubMed
-
- Sans-Coma V, Duran AC, Fernandez B, Fernandez MC, Lopez D, Arque JM. Coronary artery anomalies and bicuspid aortic valve. In: Angelini P, editor. Coronary artery anomalies: a comprehensive approach. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 17–25.
-
- Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992;20:640–7. - PubMed
-
- Virmani R, Burke AP, Farb A. The pathology of sudden cardiac death in athletes. In: Williams RA, editor. The athlete and heart disease: diagnosis, evaluation and management. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 249–72.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources