

Surgical treatment of coronary artery anomalies: report of a 37 1/2-year experience at the Texas Heart Institute
- PMID: 12484614
- PMCID: PMC140292
Surgical treatment of coronary artery anomalies: report of a 37 1/2-year experience at the Texas Heart Institute
Abstract
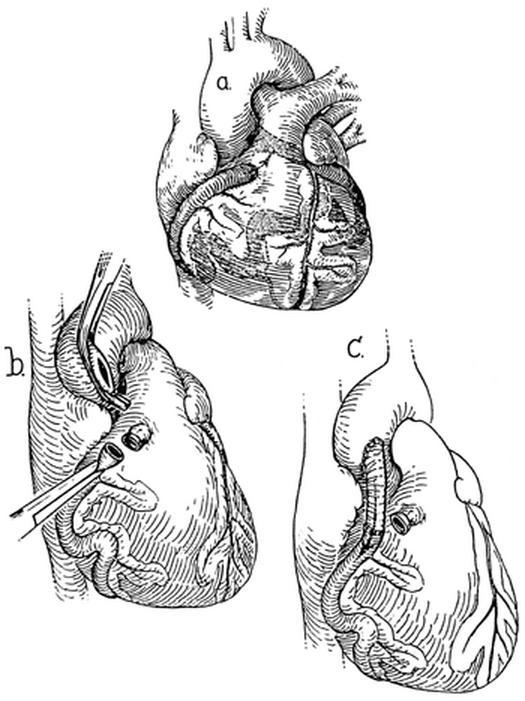
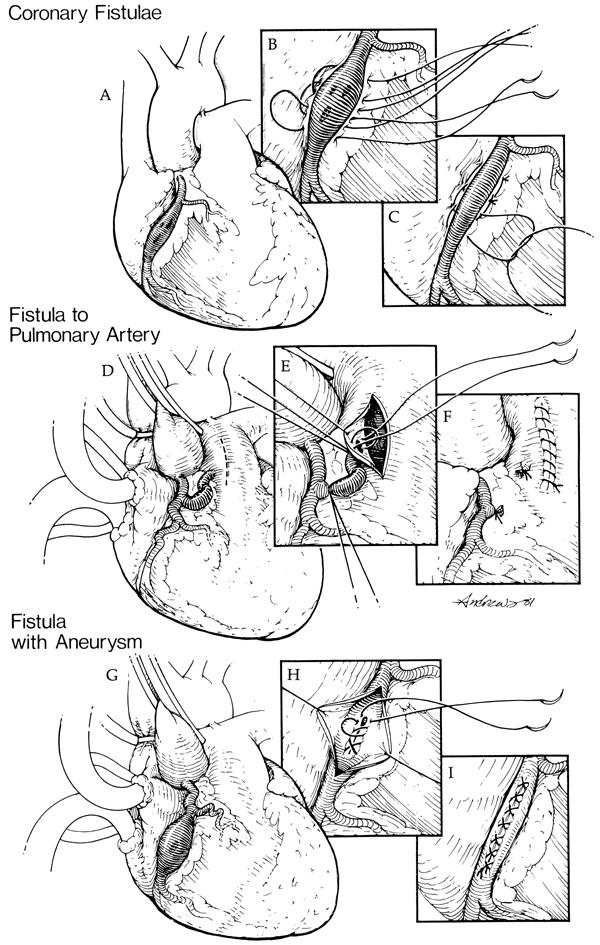
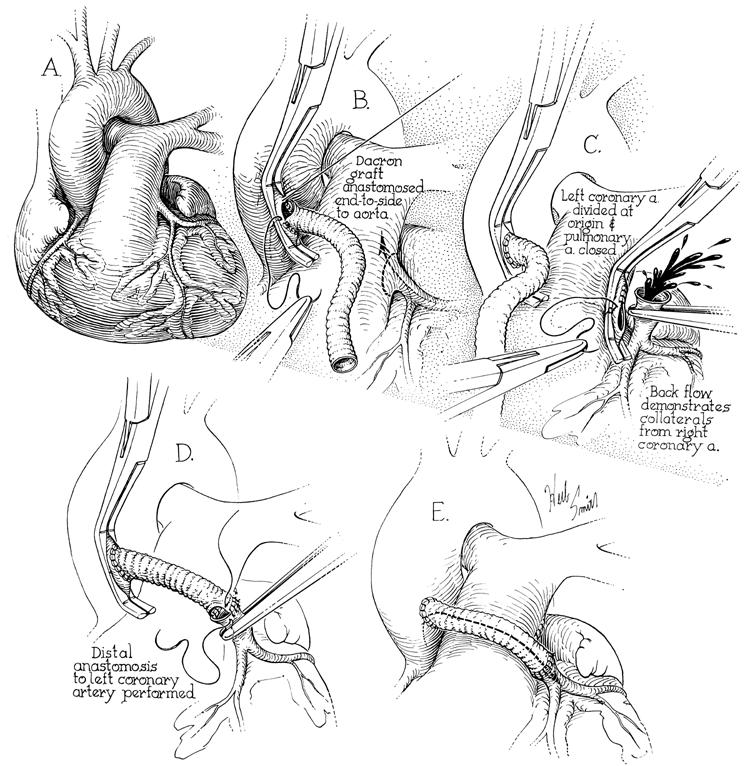
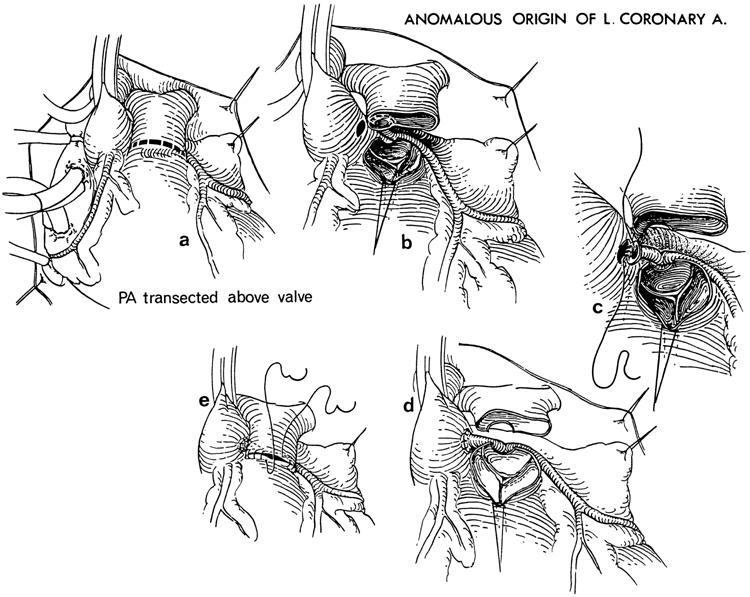
The surgical treatment of coronary artery anomalies continues to evolve. The most common coronary artery anomalies requiring surgical intervention include coronary artery fistulae, anomalous pulmonary origins of the coronary arteries, and anomalous aortic origins of the coronary arteries. The choice of surgical intervention for each type of coronary anomaly depends on several anatomic, physiologic, and patient-dependent variables. As surgical techniques have progressed, outcomes have continued to improve, however, controversy still exists about many aspects of the proper management of patients who have these coronary artery anomalies. We reviewed the surgical treatment of 178 patients who underwent surgery for the above-mentioned types of coronary artery anomalies at the Texas Heart Institute from December 1963 through June 2001. On the basis of this experience, we discuss historical aspects of the early treatment of these anomalies and describe their present-day management.
Figures
References
-
- Angelini P. Normal and anomalous coronary arteries: definitions and classification. Am Heart J 1989;117:418–34. - PubMed
-
- Dodge-Khatami A, Mavroudis C, Baker CL. Congenital Heart Surgery Nomenclature and Database Project: anomalies of the coronary arteries. Ann Thorac Surg 2000;69(4 Suppl):S270–97. - PubMed
-
- Levin DC. Anomalies and anatomic variations of the coronary arteries. In: Baum S, editor. Abrams' angiography: vascular and interventional radiology. 4th ed. Boston: Little, Brown; 1997. p. 740–55.
-
- Hallman GL, Cooley DA, McNamara DG, Latson JR. Single left coronary artery with fistula to right ventricle. Reconstruction of two-coronary system with Dacron graft. Circulation 1965;32:293–7. - PubMed
-
- Cooley DA, Ellis PR Jr. Surgical considerations of coronary arterial fistula. Am J Cardiol 1962;10:467–74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials