

Clinical review: Myocardial depression in sepsis and septic shock
- PMID: 12493071
- PMCID: PMC153435
- DOI: 10.1186/cc1822
Clinical review: Myocardial depression in sepsis and septic shock
Abstract
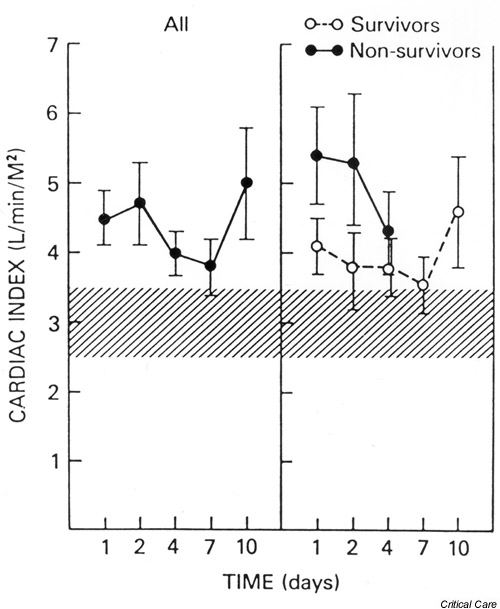
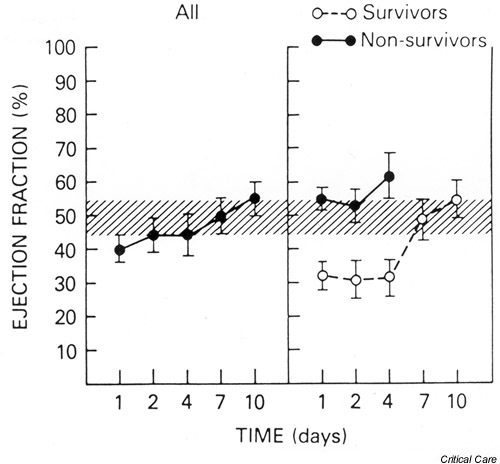
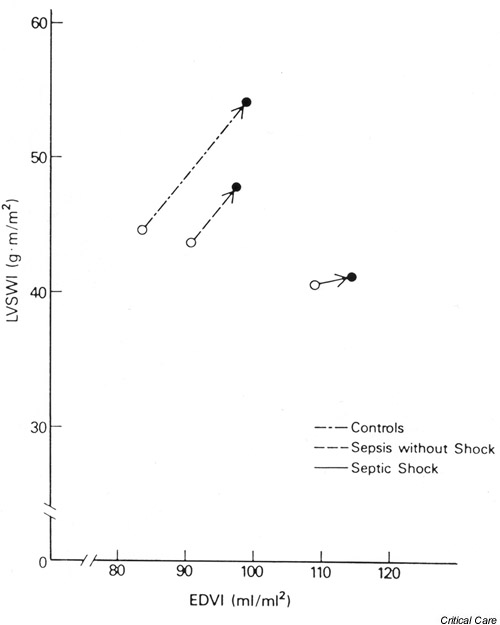
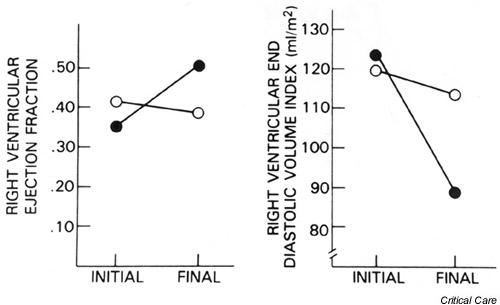
Myocardial dysfunction frequently accompanies severe sepsis and septic shock. Whereas myocardial depression was previously considered a preterminal event, it is now clear that cardiac dysfunction as evidenced by biventricular dilatation and reduced ejection fraction is present in most patients with severe sepsis and septic shock. Myocardial depression exists despite a fluid resuscitation-dependent hyperdynamic state that typically persists in septic shock patients until death or recovery. Cardiac function usually recovers within 7-10 days in survivors. Myocardial dysfunction does not appear to be due to myocardial hypoperfusion but due to circulating depressant factors, including the cytokines tumor necrosis factor alpha and IL-1beta. At a cellular level, reduced myocardial contractility seems to be induced by both nitric oxide-dependent and nitric oxide-independent mechanisms. The present paper reviews both the clinical manifestations and the molecular/cellular mechanisms of sepsis-induced myocardial depression.
Figures
References
-
- Center for Diseases Control and Prevention National Center for Health Statistics: mortality patterns – United States, 1990. Monthly Vital Stat Rep. 1993;41:5.
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:1644–1655. - PubMed
-
- Van der Poll T, Van Deventer JH. Cytokines and anticytokines in the pathogenesis of sepsis. Infect Dis Clin North Am. 1999;13:413–426. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
