

Laparoscopic gastric banding: a minimally invasive surgical treatment for morbid obesity: prospective study of 500 consecutive patients
- PMID: 12496523
- PMCID: PMC1513972
- DOI: 10.1097/00000658-200301000-00001
Laparoscopic gastric banding: a minimally invasive surgical treatment for morbid obesity: prospective study of 500 consecutive patients
Abstract
Objective: To evaluate early and late morbidity of laparoscopic adjustable gastric banding for morbid obesity and to assess the efficacy of this procedure by analyzing its results.
Summary background data: Laparoscopic adjustable gastric banding is considered the least invasive surgical option for morbid obesity. It is effective, with an average loss of 50% of excessive weight after 2 years of follow-up. It is potentially reversible and safe; major morbidity is low and there is no mortality.
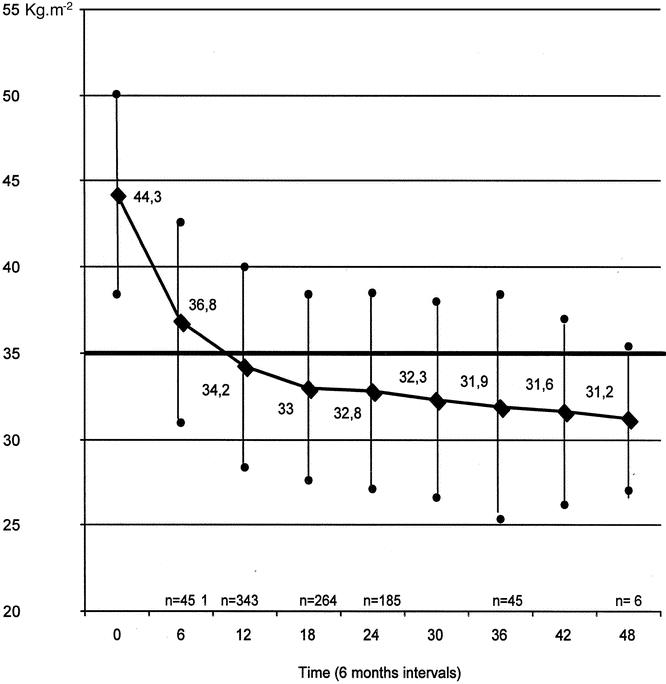
Methods: Between April 1997 and June 2001, 500 patients underwent laparoscopic surgery for morbid obesity with application of an adjustable gastric band. There were 438 women and 62 men (sex ratio = 0.14) with a mean age of 40.4 years. Preoperative mean body weight was 120.7 kg and mean body mass index (BMI) was 44.3 kg. m.
Results: Mean operative time was 105 minutes, 84 minutes during the last 300 operations. Mean hospital stay was 4.5 days. There were no deaths. There were 12 conversions (2.4%), 2 during the last 300 operations. Fifty-two patients (10.4%) had complications requiring an abdominal reoperation. Forty-nine underwent a reoperation for minor complications: slippage (n = 43, incisional hernias (n = 3), and reconnection of the catheter (n = 3). Three patients underwent a reoperation for major complications: gastroesophageal perforation (n = 2) and gastric necrosis (n = 1). Seven patients had pulmonary complications and 36 patients experienced minor problems related to the access port. At 1-, 2-, and 3-year follow-up, mean BMI decreased from 44.3 kg. m to 34.2, 32.8, and 31.9, respectively, and mean excess weight loss reached 42.8%, 52%, and 54.8%.
Conclusions: Laparoscopic adjustable gastric banding is a beneficial operation in terms of excessive weight loss, with an acceptably low complication rate. It can noticeably improve the quality of life in obese patients. Half of the excess body weight can be effortlessly lost within 2 years.
Figures




Comment on
-
Gastric banding.Ann Surg. 2003 Jan;237(1):17-8. doi: 10.1097/00000658-200301000-00003. Ann Surg. 2003. PMID: 12496525 Free PMC article. No abstract available.
References
-
- Sjöström LV. Mortality of severely obese subjects. Am J Clin Nutr 1992; 55: 516–523. - PubMed
-
- Oppert JM, Rolland-Cachera MF. Prévalence, évolution dans le temps et conséquences économiques de l’obésité. Med Sci 1998; 14: 939–943.
-
- Goodrick GK, Foreyt JP. Why treatments for obesity don’t last. JAMA 1991; 91: 1243–1247. - PubMed
-
- Mason EE, Tang S, Renquist KE, et al. A decade of change in obesity surgery. Obesity Surg 1997; 7: 189–197. - PubMed
-
- Nightengale ML, Sarr MG, Kelly KA, et al. Prospective evaluation of vertical banded gastroplasty as the primary operation for morbid obesity. Mayo Clin Proc 1991; 66: 773–782. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
