

Oncoplastic techniques allow extensive resections for breast-conserving therapy of breast carcinomas
- PMID: 12496527
- PMCID: PMC1513973
- DOI: 10.1097/00000658-200301000-00005
Oncoplastic techniques allow extensive resections for breast-conserving therapy of breast carcinomas
Abstract
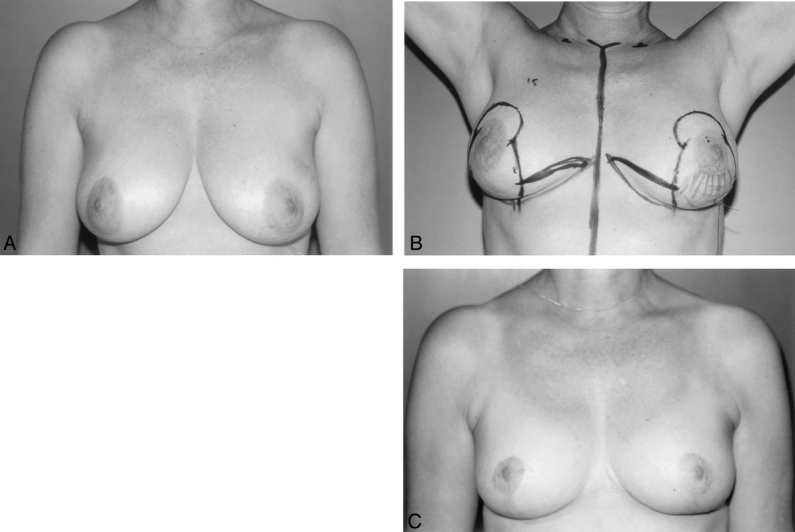
Objective: To assess the oncologic and cosmetic outcomes in women with breast carcinoma who were treated with breast-conserving therapy using oncoplastic techniques with concomitant symmetrization of the contralateral breast.
Summary background data: Although breast-conserving therapy is the standard form of treatment for invasive breast tumors up to 4 cm, in patients with large, ill-defined, or poorly situated tumors, cosmetic results can be poor and clear resection margins difficult to obtain. The integration of oncoplastic techniques with a concomitant contralateral symmetrization procedure is a novel surgical approach that allows wide excisions and prevents breast deformities.
Methods: This is a prospective study of 101 patients who were operated on for breast carcinoma between July 1985 and June 1999 at the Institut Curie. The procedure was proposed for patients in whom conservative treatment was possible on oncologic grounds but where a standard lumpectomy would have led to poor cosmesis. Standard institutional treatment protocols were followed. All patients received either pre- or postoperative radiotherapy. Seventeen patients received preoperative chemotherapy to downsize their tumors. Mean follow-up was 3.8 years. Results were analyzed statistically using Kaplan-Meier estimates.
Results: Mean weight of excised material on the tumor side was 222 g. The actuarial 5-year local recurrence rate was 9.4%, the overall survival rate was 95.7%, and the metastasis-free survival rate was 82.8%. Cosmesis was favorable in 82% of cases. Preoperative radiotherapy resulted in worse cosmesis than when given postoperatively.
Conclusions: The use of oncoplastic techniques and concomitant symmetrization of the contralateral breast allows extensive resections for conservative treatment of breast carcinoma and results in favorable oncologic and esthetic outcomes. This approach might be useful in extending the indications for conservative therapy.
Figures


References
-
- Fisher B, Anderson S, Redmond CK, et al. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1995; 333: 1456–1461. - PubMed
-
- van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst 2000; 92: 1143–1150. - PubMed
-
- Jacobson JA, Danforth DN, Cowan KH, et al. Ten-year results of a comparison of conservation with mastectomy in the treatment of stage I and II breast cancer. N Engl J Med 1995; 332: 907–911. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol 1998; 16: 441–452. - PubMed
-
- Julien JP, Bijker N, Fentiman IS, et al. Radiotherapy in breast-conserving treatment for ductal carcinoma in situ: first results of the EORTC randomised phase III trial 10853. EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. Lancet 2000; 355: 528–533. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
