

Laparoscopic staging and subsequent palliation in patients with peripancreatic carcinoma
- PMID: 12496532
- PMCID: PMC1513968
- DOI: 10.1097/00000658-200301000-00010
Laparoscopic staging and subsequent palliation in patients with peripancreatic carcinoma
Abstract
Objective: To test the hypothesis that laparoscopic staging improves outcome in patients with peripancreatic carcinoma compared to standard radiology staging.
Summary background data: Diagnostic laparoscopy of peripancreatic malignancies has been reported to improve assessment of tumor stage and to prevent unnecessary exploratory laparotomies in 10% to 76% of patients.
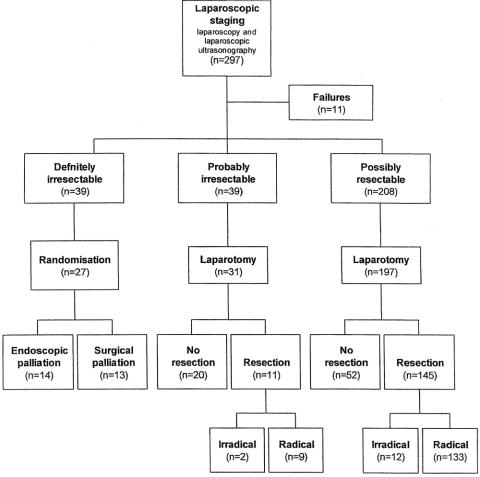
Methods: Laparoscopy and laparoscopic ultrasound were performed in 297 consecutive patients with peripancreatic carcinoma scheduled for surgery after radiologic staging. Patients with pathology-proven unresectable tumors were randomly allocated to either surgical or endoscopic palliation. All others underwent laparotomy.
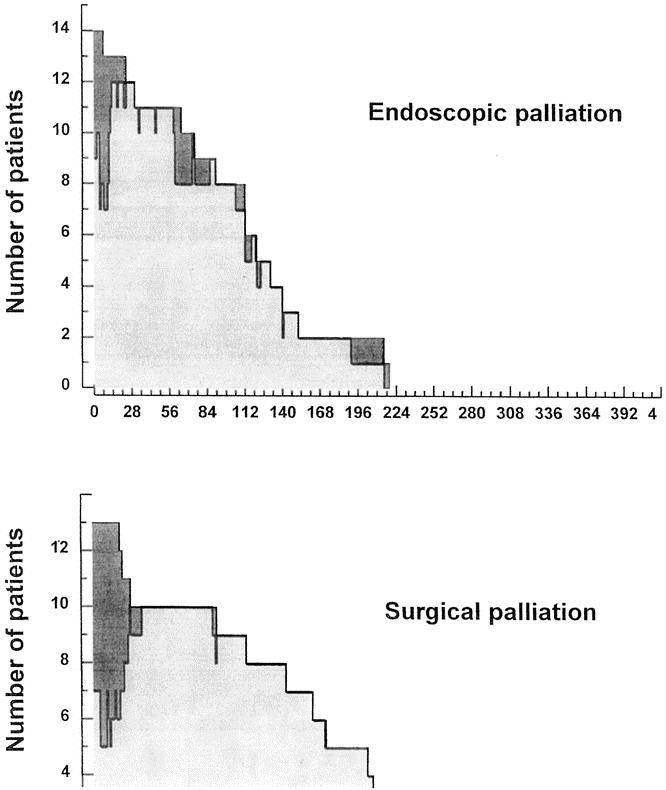
Results: Laparoscopic staging detected biopsy-proven unresectable disease in 39 patients (13%). At laparotomy, unresectable disease was found in another 72 patients, leading to a detection rate for laparoscopic staging of 35%. In total, 145 of the 197 patients classified as having "possibly resectable" disease after laparoscopic staging underwent resection (74%). Average survival in the group of 14 patients with biopsy-proven unresectable tumors randomly allocated to endoscopic palliation was 116 days, with a mean hospital-free survival of 94 days. The corresponding figures were 192 days and 164 days in the 13 patients allocated to surgical palliation.
Conclusions: Because of the limited detection rate for unresectable metastatic disease and the likely absence of a large gain after switching from surgical to endoscopic palliation, laparoscopic staging should not be performed routinely in patients with peripancreatic carcinoma.
Figures
References
-
- Warshaw AL, Tepper JE, Shipley WU. Laparoscopy in the staging and planning of therapy for pancreatic cancer. Am J Surg 1986; 151: 76–80. - PubMed
-
- Fernandez-del Castillo C, Rattner DW, Warshaw AL. Further experience with laparoscopy and peritoneal cytology in the staging of pancreatic cancer. Br J Surg 1995; 82: 1127–1129. - PubMed
-
- Babineau TJ, Lewis WD, Jenkins RL, et al. Role of Staging Laparoscopy in the Treatment of Hepatic Malignancy. Am J Surg 1994; 167: 151–155. - PubMed
-
- Stein HJ, Kraemer SJM, Feussner H, et al. Clinical value of diagnostic laparoscopy with laparoscopic ultrasound in patients with cancer of the esophagus or cardia. J Gastrointestinal Surg 1997; 1: 167–173. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
