

Prognostic factors following curative resection for pancreatic adenocarcinoma: a population-based, linked database analysis of 396 patients
- PMID: 12496533
- PMCID: PMC1513971
- DOI: 10.1097/00000658-200301000-00011
Prognostic factors following curative resection for pancreatic adenocarcinoma: a population-based, linked database analysis of 396 patients
Abstract
Objective: To analyze prognostic factors influencing pancreatic cancer survival following curative resection, using prospectively collected, population-based data.
Summary background data: Several studies have analyzed the determinants of long-term survival in postresection pancreatic cancer patients, but the majority of these have been single-institutional chart reviews yielding inconsistent results.
Methods: This retrospective cohort study examined 396 Medicare-eligible patients over age 65 who were diagnosed with nonmetastatic pancreatic adenocarcinoma and who underwent surgical resection with curative intent while residing in one of the 11 Survival, Epidemiology, and End Results (SEER) registries between January 1991 and December 1996. Linked Medicare data provided information on treatment and comorbidity, while linked census tract data supplied sociodemographic characteristics.
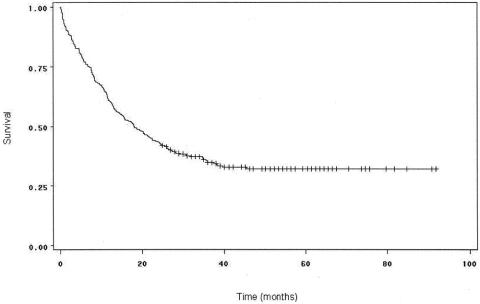
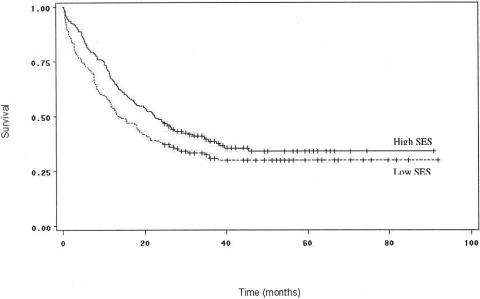
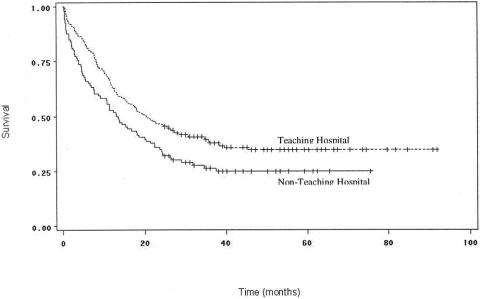
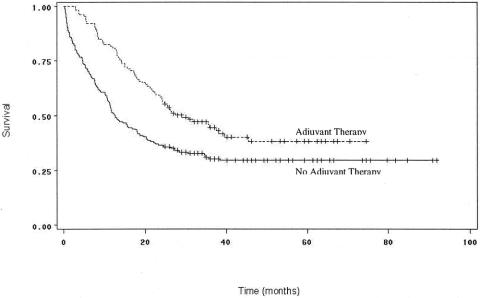
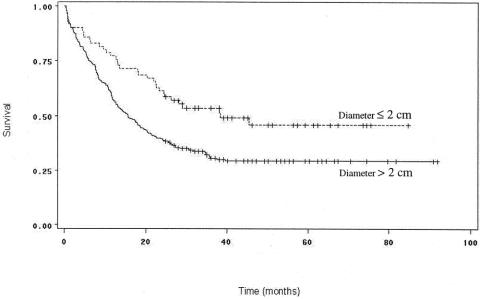
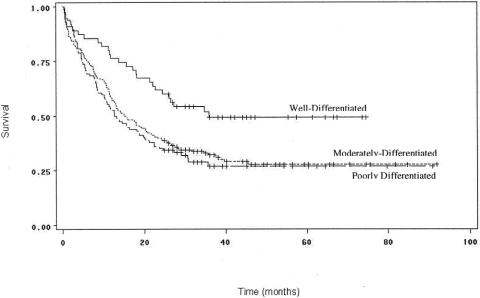
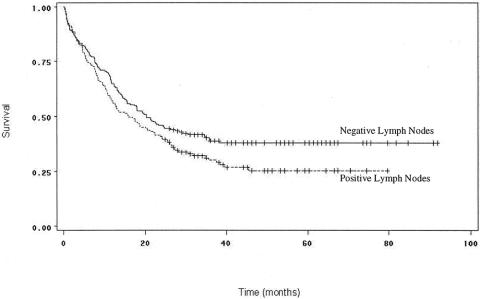
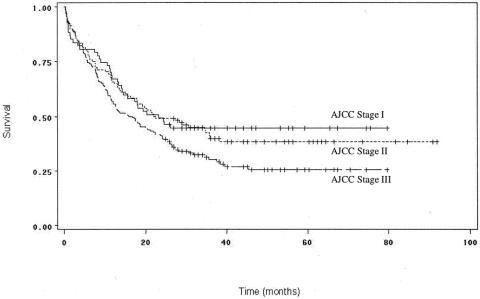
Results: Median survival for the overall study population was 17.6 months, with 1- and 3-year survival rates of 60.1% and 34.3%, respectively. Survival appears to be gradually improving over time, concomitant with a rise in the proportion of patients undergoing surgery in teaching centers. Prognostic variables significantly diminishing survival on univariate analysis included African American race, treatment not in a teaching hospital, lack of adjuvant chemoradiation therapy, as well as histopathologic factors that included tumor size larger than 2 cm in diameter, moderate to poor histologic grade, and positive lymph node metastases. Higher socioeconomic status was associated both with an increased likelihood of receiving adjuvant therapy and improved overall survival. Multivariate analyses indicated the strongest predictors of survival were adjuvant combined chemoradiotherapy, small tumors (<2 cm in diameter), negative lymph nodes, well-differentiated histology, undergoing surgery in a teaching hospital, and high socioeconomic status.
Conclusions: Although biologic characteristics remain important predictors of survival for patients with resected pancreatic cancer, the most powerful determinant is postoperative adjuvant chemoradiation therapy. An interesting finding that warrants further investigation is the effect of socioeconomic status on both the likelihood of receiving adjuvant treatment and subsequent survival, indicating a possible relationship between the quality of care delivered and outcomes.
Figures
References
-
- Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics, 1999. CA Cancer J Clin 1999; 49: 8–31. - PubMed
-
- National Cancer Institute. SEER cancer statistics review 1973–1996. NIH Publication No. 99–2789. Bethesda, Department of Health and Human Services, 1999.
-
- Brennan MF, Kinsella TJ, Casper ES. Cancer of the pancreas. In De Vita VT, Helmann S, Rosenberg SA, eds. Cancer: principles & practice of oncology. Philadelphia: JB Lippincott; 1993: 849–882.
-
- Reber HA, Gloor B. Radical pancreatectomy. Surg Oncol Clin North Am 1998; 7: 157–163. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA 1998; 280: 1747–1751. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
