

Deletion of RD1 from Mycobacterium tuberculosis mimics bacille Calmette-Guérin attenuation
- PMID: 12508154
- PMCID: PMC1458498
- DOI: 10.1086/345862
Deletion of RD1 from Mycobacterium tuberculosis mimics bacille Calmette-Guérin attenuation
Abstract
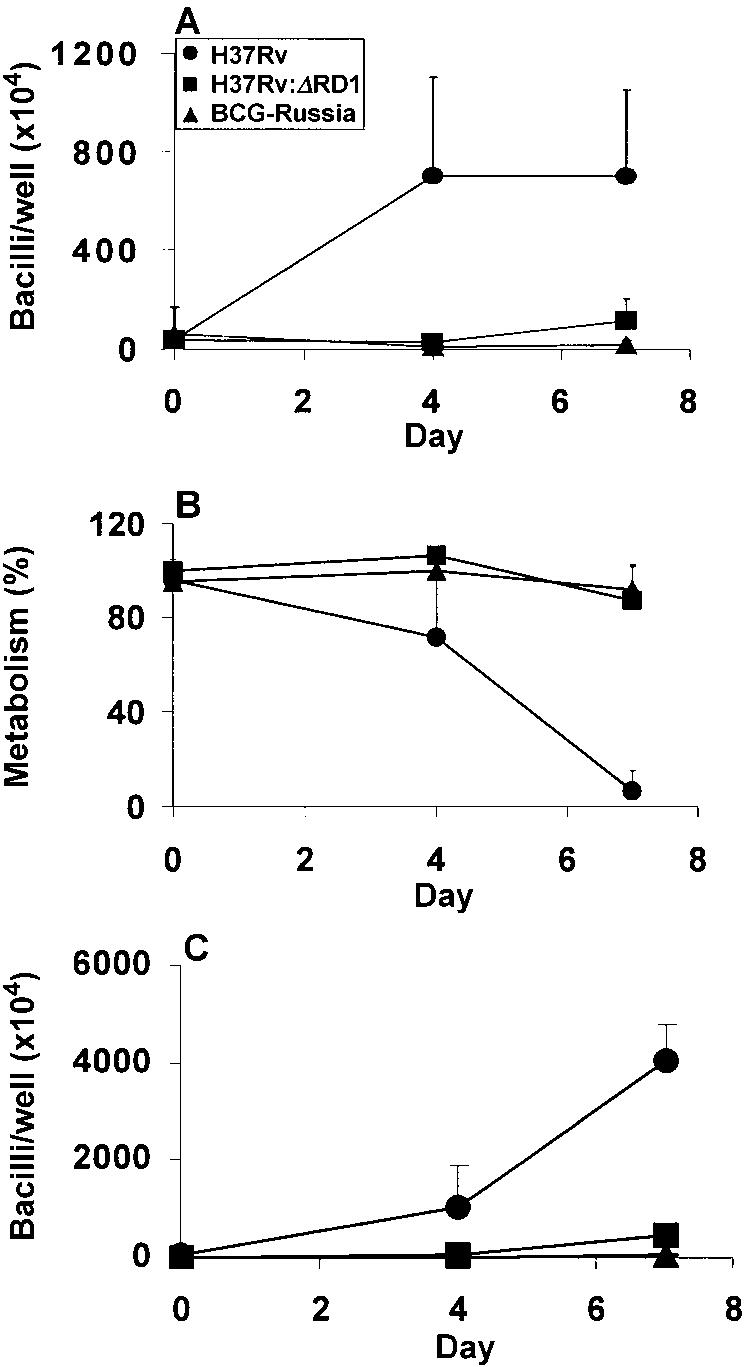
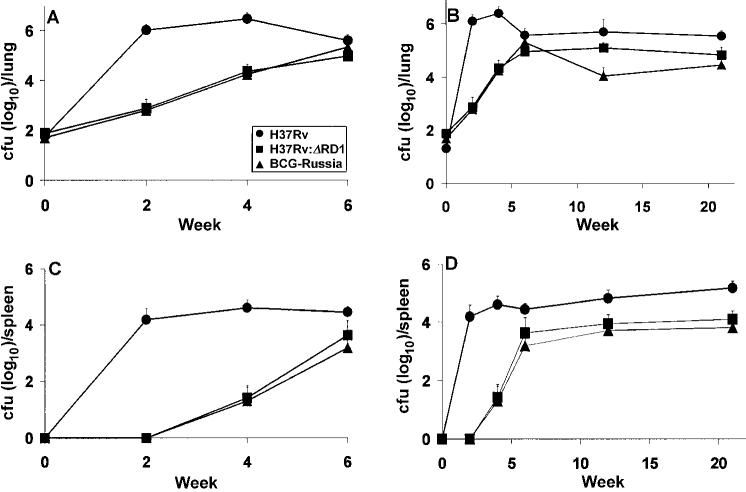
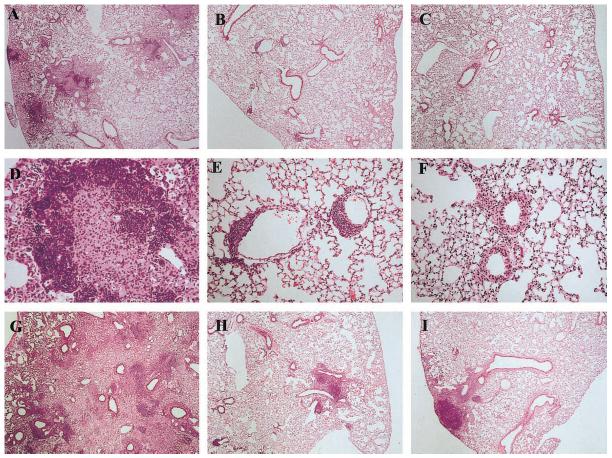
The tuberculosis (TB) vaccine bacille Calmette-Guérin (BCG) is a live attenuated organism, but the mutation responsible for its attenuation has never been defined. Recent genetic studies identified a single DNA region of difference, RD1, which is absent in all BCG strains and present in all Mycobacterium tuberculosis (MTB) strains. The 9 open-reading frames predicted within this 9.5-kb region are of unknown function, although they include the TB-specific immunodominant antigens ESAT-6 and CFP-10. In this study, RD1 was deleted from MTB strain H37Rv, and virulence of H37Rv:DeltaRD1 was assessed after infections of the human macrophage-like cell line THP-1, human peripheral blood monocyte-derived macrophages, and C57BL/6 mice. In each of these systems, the H37Rv:DeltaRD1 strain was strikingly less virulent than MTB and was very similar to BCG controls. Therefore, it was concluded that genes within or controlled by RD1 are essential for MTB virulence and that loss of RD1 was important in BCG attenuation.
Figures
References
-
- Bloom BR, Fine PEM. The BCG experience: implications for future vaccines against tuberculosis. In: Bloom BR, editor. Tuberculosis: pathogenesis, protection, and control. American Society for Microbiology Press; Washington, DC: 1994. pp. 531–57.
-
- Fine PEM, Carneiro IAM, Milstien JB, Clements CJ. Issues relating to the use of BCG in immunization programmes. Available at: http://www.who.int/vaccines-documents/DocsPDF99/www9943.pdf . Last accessed 15 November 2002.
-
- Casanova JL, Blanche S, Emile JF, et al. Idiopathic disseminated bacillus Calmette-Guérin infection: a French national retrospective study. Pediatrics. 1996;98:774–8. - PubMed
-
- Huebner RE. Bacillus of the Calmette and Guérin (BCG) vaccine. In: Rom WN, Garay SM, editors. Tuberculosis. Little, Brown & Company; Boston: 1996. pp. 893–904.
-
- Zumla A, Mwaba P, Squire SB, Grange JM. The tuberculosis pandemic: which way now? J Infect. 1999;38:74–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
