

Fetal cytomegalovirus infection of the brain: the spectrum of sonographic findings
- PMID: 12533323
- PMCID: PMC8148945
Fetal cytomegalovirus infection of the brain: the spectrum of sonographic findings
Abstract
Background and purpose: Congenital cytomegalovirus (CMV) infection can cause a wide range of brain anomalies. These changes have been well described postnatally, but descriptions of their in utero evolution are scarce. The purpose of this study was to analyze the sonographic spectrum of intracranial abnormalities in fetuses with proved CMV infection and to determine characteristic patterns of this infection.
Methods: We reviewed the transabdominal and transvaginal sonograms of eight fetuses with proved CMV infection. The sonographic analysis searched for signs of ventriculitis, leukomalacia, calcification, vasculitis, and periventricular cyst formation. The gyral pattern, corpus callosum, and cerebellar morphology also were examined. Fetal MR imaging was performed in two cases.
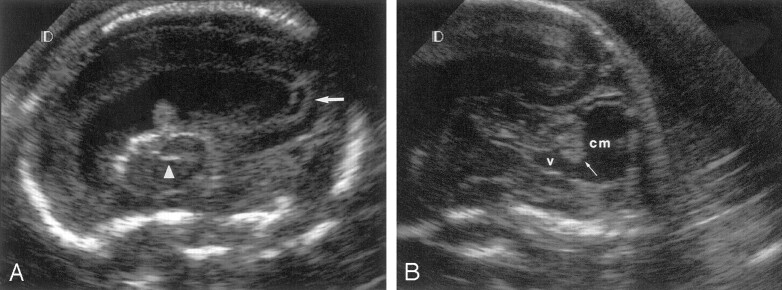
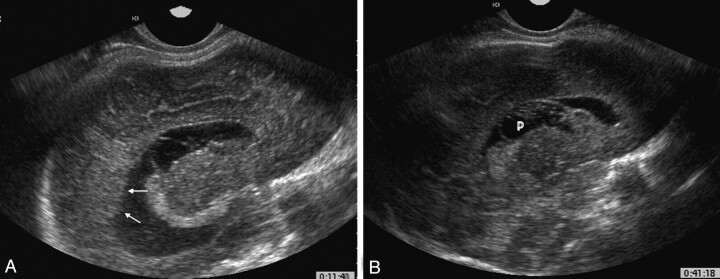
Results: The sonographic diagnosis of suspected CMV infection was made at a mean gestational age of 27.5 weeks (range, 22-37 weeks). An abnormal pattern of periventricular echogenicity was found in all fetuses. Echogenic intraparenchymal foci and ventriculomegaly were present in five fetuses. Other signs of fetal infection were intraventricular adhesions, periventricular pseudocysts, sulcation and gyral abnormal patterns, hypoplastic corpus callosum, cerebellar and cisterna magna abnormalities, and signs of striatal artery vasculopathy. For all fetuses, transvaginal sonography provided additional information. Fetal MR imaging provided additional information in one case.
Conclusion: The presence of the described sonographic findings, particularly if two or more are present in the same fetus, is an indication for CMV investigation.
Figures



References
-
- Demmler GJ, Infectious Diseases Society of America and Centers for Disease Control. Summary of a workshop on surveillance for congenital cytomegalovirus disease. Rev Infect Dis 1991;13:315–329 - PubMed
-
- Istas AS, Demmler GJ, Dobbins JG, Stewart JA. Surveillance for congenital cytomegalovirus disease: a report from the National Congenital Cytomegalovirus Disease Registry. Clin Infect Dis 1995;20:665–670 - PubMed
-
- Uziel Y, Shahar G, Regev R, Dolfin Z. CMV infections in the mother and newborn. Harefuah 1991;120:536–539 - PubMed
-
- Yow MD, Williamson DW, Leeds LJ, at al. Epidemiologic characteristics of cytomegalovirus infection in mothers and their infants. Am J Obstet Gynecol 1988;158:1189–1195 - PubMed
-
- Stagno S, Pass RF, Cloud G, et al. Primary cytomegalovirus infection in pregnancy: incidence, transmission to fetus, and clinical outcome. JAMA 1986;256:1904–1908 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical