

Thromboembolic events associated with Guglielmi detachable coil embolization of asymptomatic cerebral aneurysms: evaluation of 66 consecutive cases with use of diffusion-weighted MR imaging
- PMID: 12533341
- PMCID: PMC8148978
Thromboembolic events associated with Guglielmi detachable coil embolization of asymptomatic cerebral aneurysms: evaluation of 66 consecutive cases with use of diffusion-weighted MR imaging
Abstract
Background and purpose: Although Guglielmi detachable coil (GDC) endovascular treatment of intracranial aneurysms has become an accepted alternative to surgery, the main complication continues to be thromboembolic events. We sought to determine the frequency and radiologic appearance of thromboembolic events during GDC embolization for asymptomatic cerebral aneurysms by using diffusion-weighted (DW) MR imaging and to determine whether aneurysmal anatomic factors or use of the balloon-assisted technique affected the frequency.
Methods: In 74 patients, 79 asymptomatic cerebral aneurysms were treated with GDC embolizations at the National Cardiovascular Center from 1999 to 2001. Thirty-nine of these aneurysms (49%) were treated with the balloon-assisted technique. DW imaging was performed in 66 patients at 2-5 days after GDC embolization. All DW images were reviewed by two radiologists for depiction of abnormalities.
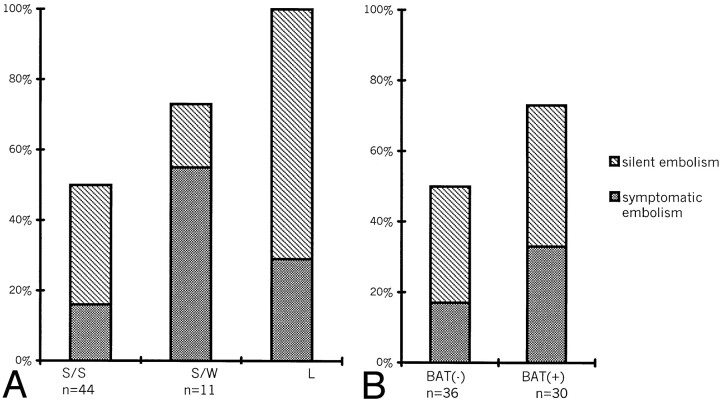
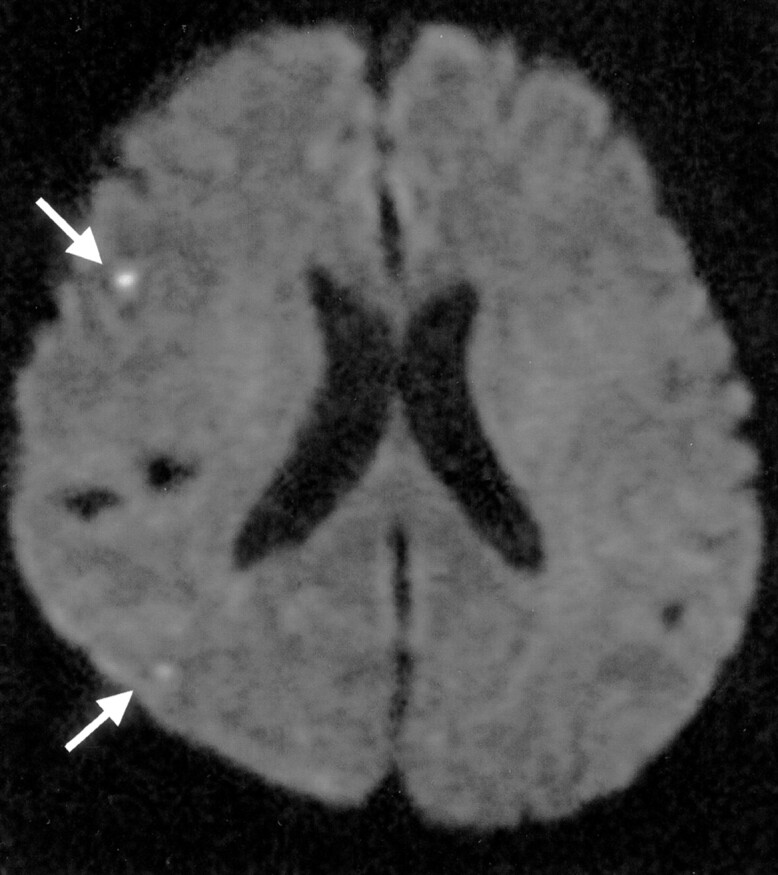
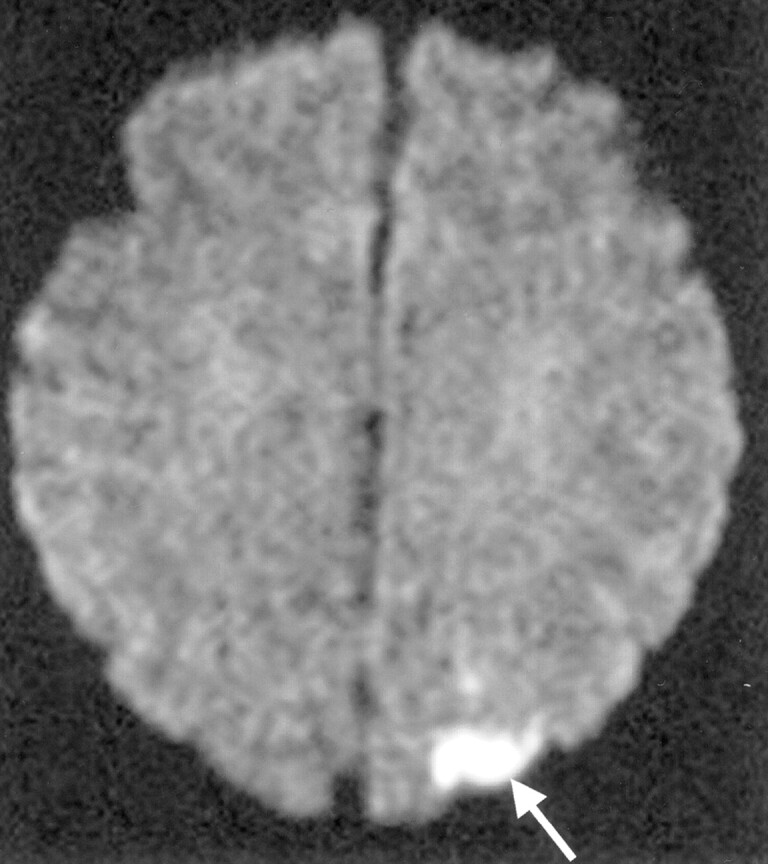
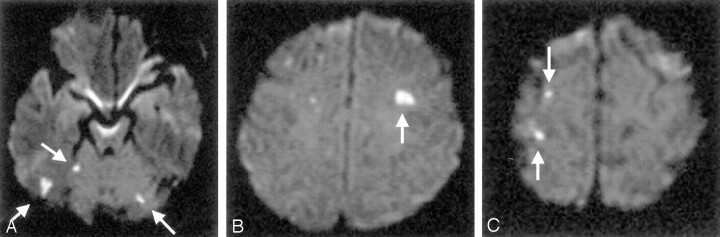
Results: DW images showed hyperintense lesions in 40 patients (61%), with 16 of these patients (40%) incurring neurologic deteriorations. Fifteen of the symptomatic patients (94%) fully recovered by discharge, and the remaining one experienced permanent deficits. Hyperintense lesions were detected more frequently in wide-neck (73%) or large (100%) aneurysms and in procedures that used the balloon-assisted technique (73%) than in small aneurysms (50%) or in procedures with the simple GDC method (49%). The occurrence of new lesions was significantly associated with use of the balloon-assisted technique and with aneurysm diameter in multivariate analysis (P <.05).
Conclusion: In our experience, thromboembolic events related to the use of GDC embolization are relatively common, especially in wide-neck or large aneurysms or in association with the balloon-assisted technique. Although permanent deficits are rare, the high rate of thromboembolic events suggests that improvements in the technique such as the addition of antiplatelet agents and the development of new embolic materials are mandatory.
Figures
Comment in
-
Thromboembolic events associated with Guglielmi detachable coil embolization of asymptomatic cerebral aneurysms: evaluation of 66 consecutive cases with use of diffusion-weighted MR imaging.AJNR Am J Neuroradiol. 2004 Jan;25(1):159-60; author reply 160. AJNR Am J Neuroradiol. 2004. PMID: 14729550 Free PMC article. No abstract available.
-
Diffusion-weighted imaging of thromboembolic events associated with coil embolization of intracranial aneurysms.AJNR Am J Neuroradiol. 2004 Nov-Dec;25(10):1861; author reply 1861-2. AJNR Am J Neuroradiol. 2004. PMID: 15569765 Free PMC article. No abstract available.
References
-
- Guglielmi G, Vinuela F, Dion J. Electrothrombosis of saccular aneurysms via endovascular approach, II: preliminary clinical experience. J Neurosurg 1991;75:8–14 - PubMed
-
- Vinuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475–482 - PubMed
-
- Murayama Y, Vinuela F, Duckwiler GR, Gobin YP, Guglielmi G. Embolizatiion of incidental cerebral aneurysms by using the Guglielmi detachable coil system. J Neurosurg 1999;90:207–214 - PubMed
-
- Moret J, Cognard C, Weill A, Castaings L, Rey A. The “remodeling technique” in the treatment of wide neck intracranial aneurysms. Intervent Neuroradiol 1997;3:21–35 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical