

Screening for diabetic retinopathy in James Bay, Ontario: a cost-effectiveness analysis
- PMID: 12538543
- PMCID: PMC140424
Screening for diabetic retinopathy in James Bay, Ontario: a cost-effectiveness analysis
Abstract
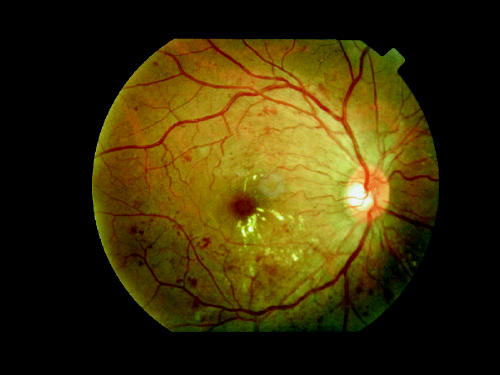
Background: Retinopathy is a common complication of diabetes mellitus that if detected early by regular retinal examinations can be treated; thus, blindness can be delayed or prevented. Providing high-quality retinal screening is difficult, especially in rural and remote areas. Canada's First Nations population has a higher prevalence of diabetes and is, in general, more geographically isolated than the broader Canadian population. We modelled the cost-effectiveness of retinopathy screening by travelling retina specialists versus retinal photography with a portable digital camera in an isolated First Nations cohort with diabetes.
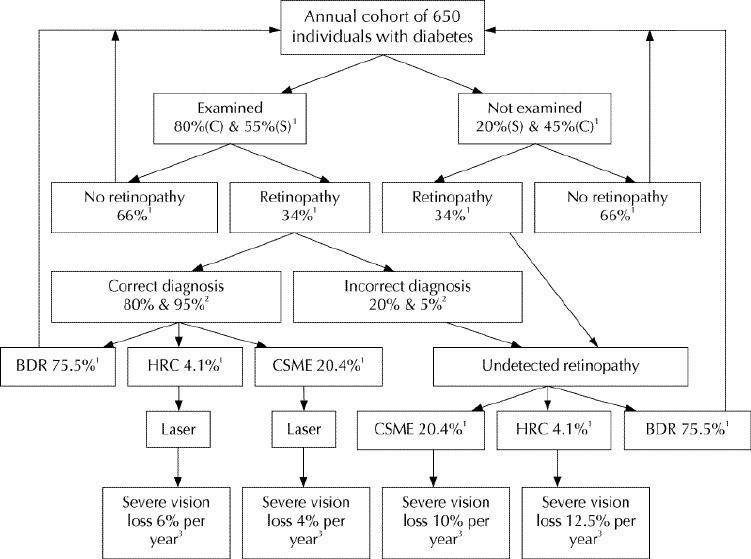
Methods: The 2 screening programs were modelled to run concurrently for 5 years, with outcomes evaluated over 10 years. To construct economic models for the population of Cree individuals living in the western James Bay area of northern Ontario, we used available data on the prevalence of diabetes in the area and estimates of the incidence of retinopathy derived from the published literature. We compared the screening models and calculated total costs, visual outcome, costs per sight-year saved and costs per quality-adjusted life year (QALY). We also estimated the costs of implementing a screening program for all First Nations individuals in Ontario with diabetes and no access to an ophthalmologist.
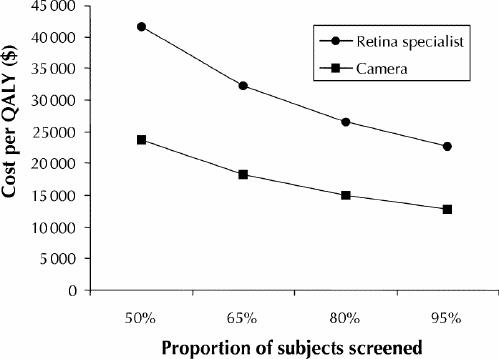
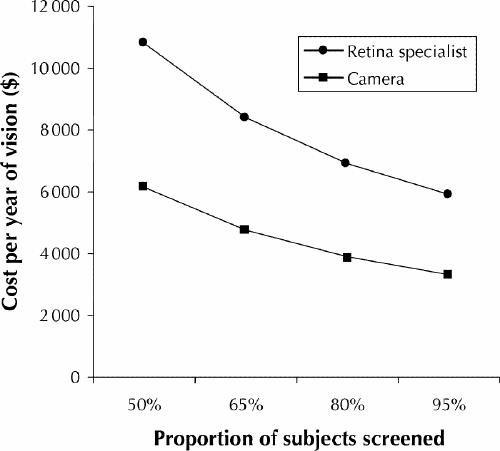
Results: From the perspective of the health care system the camera program was preferable to the specialist-based program. Over 10 years, 67 v. 56 sight years were saved, compared with no screening, at costs of 3900 Canadian dollars v. 9800 Canadian dollars per sight year and 15,000 Canadian dollars v. 37,000 Canadian dollars per QALY. Generalizing these results to the province of Ontario, the camera system could allow most isolated First Nations people with diabetes to be screened for 5 years for approximately 1.2 million Canadian dollars.
Interpretation: A portable retinal camera is a cost-effective means of screening for diabetic retinopathy in isolated communities of at-risk individuals.
Figures
References
-
- Wisconsin Epidemiologic Study of Diabetic Retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch Ophthalmol 1984;102:527-32. - PubMed
-
- Maberley D, King W, Cruess A. Prevalence of diabetes in the Cree of Western James Bay. Chronic Dis Can 2000;21:128-33. - PubMed
-
- Evers S, McCracken E, Antone I, Deagle G. The prevalence of diabetes in Indians and Caucasians living in Southwestern Ontario. Can J Public Health 1987; 78:240-3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical