

Diagnosis of pulmonary embolism
- PMID: 12538548
- PMCID: PMC140429
Diagnosis of pulmonary embolism
Abstract
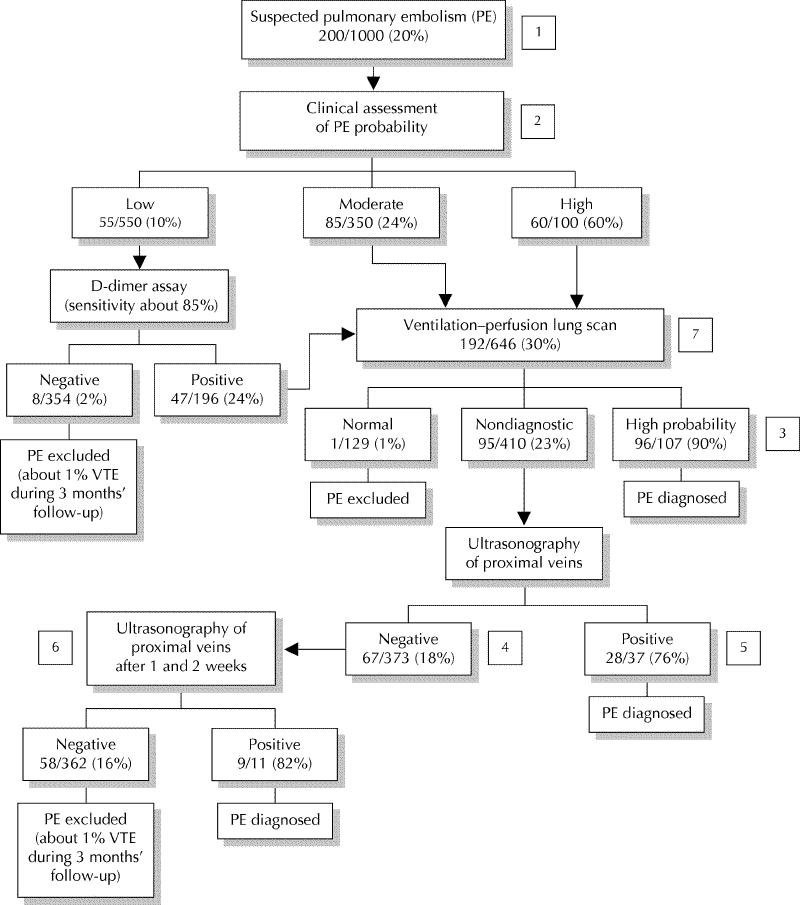
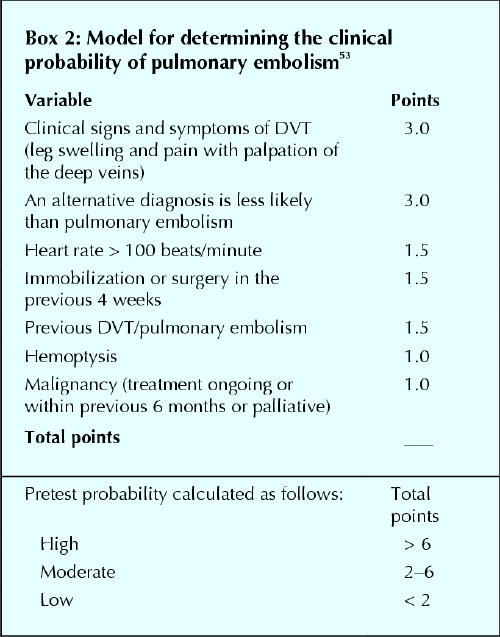
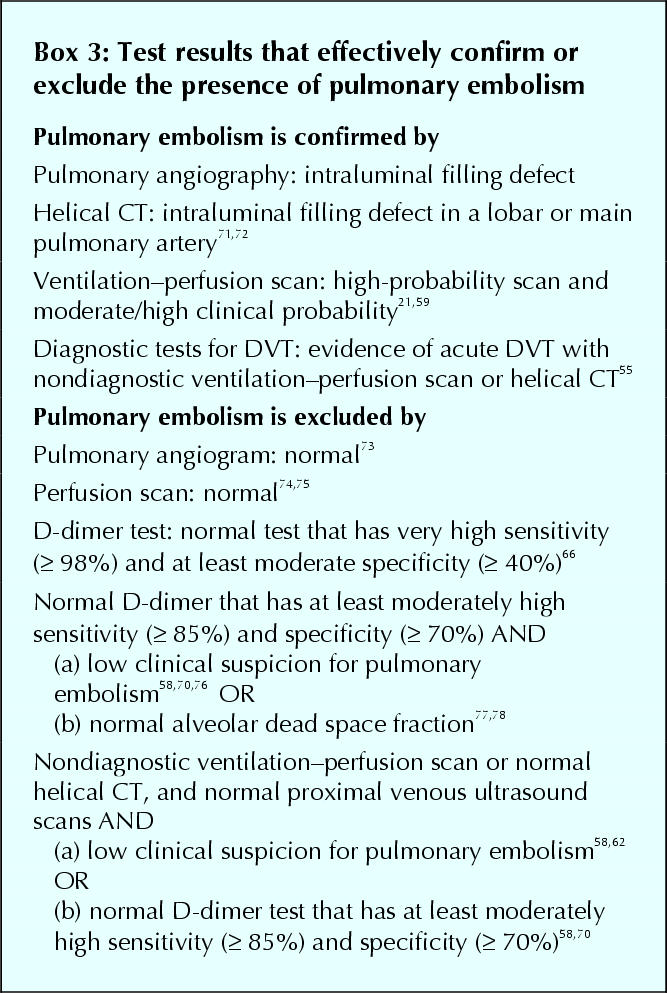
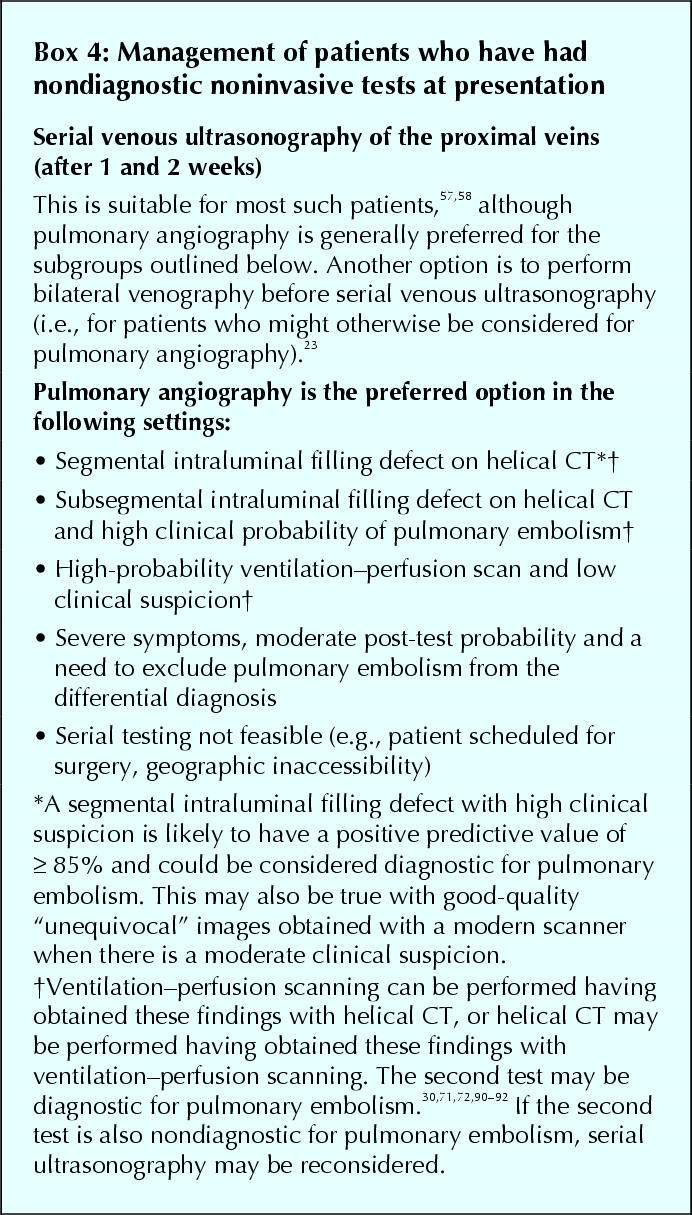
No single noninvasive test for pulmonary embolism is both sensitive and specific. Some tests are good for "ruling in" pulmonary embolism (e.g., helical CT) and some tests are good for "ruling out" pulmonary embolism (e.g., D-dimer); others are able to do both but are often nondiagnostic (e.g., ventilation-perfusion lung scanning). For optimal efficiency, choice of the initial diagnostic test should be guided by clinical assessment of the probability of pulmonary embolism and by patient characteristics that may influence test accuracy. This selective approach to testing enables pulmonary embolism to be diagnosed or excluded in a minimum number of steps. However, even with the appropriate use of combinations of noninvasive tests, it is often not possible to definitively diagnose or exclude pulmonary embolism at initial presentation. Most of these patients can be managed safely without treatment or pulmonary angiography by repeating ultrasound testing of the proximal veins after one and 2 weeks to detect evolving deep vein thrombosis. Helical CT and MRI are rapidly improving as diagnostic tests for pulmonary embolism and are expected to become central to its evaluation.
Figures

Comment in
-
Excluding pulmonary embolism with helical (spiral) computed tomography: Evidence is catching up with enthusiasm.CMAJ. 2003 May 27;168(11):1430-1. CMAJ. 2003. PMID: 12771073 Free PMC article. No abstract available.
References
-
- Pineda LA, Hathwar VS, Grant BJ. Clinical suspicion of fatal pulmonary embolism. Chest 2001;120:791-5. - PubMed
-
- Kearon C. Natural history of venous thromboembolism. Semin Vasc Med 2001; 1:27-37. - PubMed
-
- Kakkar VV, Howe CT, Flanc C, Clarke MB. Natural history of postoperative deep-vein thrombosis. Lancet 1969;2:230-2. - PubMed
-
- Nicolaides AN, Kakkar VV, Field ES, Renney JTG. The origin of deep vein thrombosis: a venographic study. Br J Radiol 1971;44:653-63. - PubMed
-
- Cogo A, Lensing AWA, Prandoni P, Hirsh J. Distribution of thrombosis in patients with symptomatic deep-vein thrombosis: implications for simplifying the diagnostic process with compression ultrasound. Arch Intern Med 1993; 153: 2777-80. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical