

Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity
- PMID: 12542581
- PMCID: PMC1494814
- DOI: 10.1046/j.1525-1497.2003.20441.x
Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity
Abstract
Objective: To examine if delayed transfer to the intensive care unit (ICU) after physiologic deterioration is associated with increased morbidity and mortality.
Design: Inception cohort.
Setting: Community hospital in Ogden, Utah.
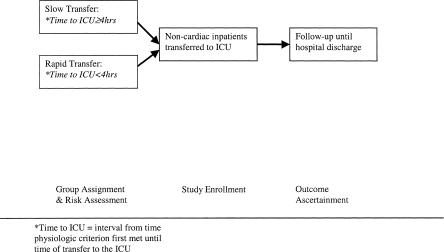
Patients: Ninety-one consecutive inpatients with noncardiac diagnoses at the time of emergent transfer to the ICU. We determined the time when each patient first met any of 11 pre-specified physiologic criteria. We classified patients as "slow transfer" when patients met a physiologic criterion 4 or more hours before transfer to the ICU. Patients were followed until discharge.
Interventions: None.
Measurements: In-hospital mortality, functional status at hospital discharge, hospital resources.
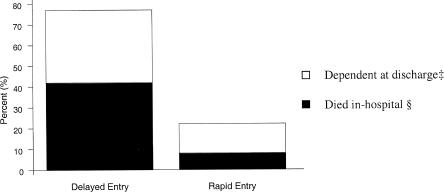
Main results: At the time when the first physiologic criterion was met on the ward, slow- and rapid-transfer patients were similar in terms of age, gender, diagnosis, number of days in hospital prior to ICU transfer, prehospital functional status, and APACHE II scores. By the time slow-transfer patients were admitted to the ICU, they had significantly higher APACHE II scores (21.7 vs 16.2; P =.002) and were more likely to die in-hospital (41% vs 11%; relative risk [RR], 3.5; 95% confidence interval [95% CI], 1.4 to 9.5). Slow-transfer patients were less likely to have had their physician notified of deterioration within 2 hours of meeting physiologic criteria (59% vs 31%; P =.001) and less likely to have had a bedside physician evaluation within the first 3 hours after meeting criteria (23% vs 83%; P =.001).
Conclusions: Slow transfer to the ICU of physiologically defined high-risk hospitalized patients was associated with increased risk of death. Slow response to physiologic deterioration may explain these findings.
Figures
Comment on
-
Delays in transfer to the ICU: a preventable adverse advent?J Gen Intern Med. 2003 Feb;18(2):155-6. doi: 10.1046/j.1525-1497.2003.21217.x. J Gen Intern Med. 2003. PMID: 12542592 Free PMC article. No abstract available.
References
-
- Zimmerman JE, Wagner DP, Draper EA, Wright L, Alzola C, Knaus WA. Evaluation of acute physiology and chronic health evaluation III predictions of hospital mortality in an independent database. Crit Care Med. 1998;26:1317–26. - PubMed
-
- Lundberg JS, Perl TM, Wiblin T, Costigan MD, Dawson J, Nettelman MD, Wenzel RP. Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units. Crit Care Med. 1988;26:1020–4. - PubMed
-
- Rapoport J, Teres D, Lemeshow S, Harris D. Timing of intensive care unit admission in relation to ICU outcome. Crit Care Med. 1990;18:1231–6. - PubMed
-
- Berensen RA. Office of Technology Assessment Case Study 28. Washington DC: U.S. Government Printing Office; 1984. Intensive Care Units (ICU's) Clinical Outcomes, Costs and Decision Making.
-
- Oye RK, Bellamy PF. Patterns of resource consumption in medical intensive care. Chest. 1991;99:685–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous