

doi: 10.1046/j.1525-1497.2003.20532.x.
Racial and ethnic disparities in the use of health services: bias, preferences, or poor communication?
Affiliations
- PMID: 12542590
- PMCID: PMC1494820
- DOI: 10.1046/j.1525-1497.2003.20532.x
Item in Clipboard
Racial and ethnic disparities in the use of health services: bias, preferences, or poor communication?
J Gen Intern Med.
2003 Feb.
Abstract
African Americans and Latinos use services that require a doctor's order at lower rates than do whites. Racial bias and patient preferences contribute to disparities, but their effects appear small. Communication during the medical interaction plays a central role in decision making about subsequent interventions and health behaviors. Research has shown that doctors have poorer communication with minority patients than with others, but problems in doctor-patient communication have received little attention as a potential cause, a remediable one, of health disparities. We evaluate the evidence that poor communication is a cause of disparities and propose some remedies drawn from the communication sciences.
Figures
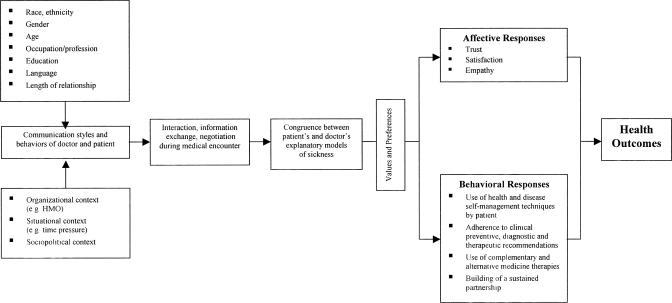
Proposed conceptual framework for how race and ethnicity affect the communication patterns of patient and doctor, their attempts to understand each other's explanatory models for the sickness, and their ability to negotiate to congruence between the respective models. Communication drives the achievement or lack of congruence between the explanatory models. The extent to which the patient and doctor develop congruence between their respective models affects affective and behavioral responses on the part of the patient. In turn, these affective and behavioral responses affect health outcomes.
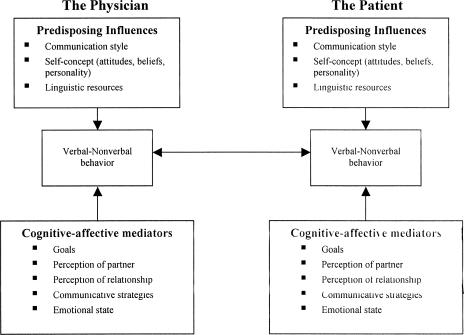
Processes related to communicative consistency or adaptation. Predisposing factors lead to consistency in communicative behaviors, but cognitive-affective mediators, among them communicative strategies, lead partners to adapt their communicative behaviors to each other. Communicative strategies on the part of the patient, including telling a health narrative, asking questions, expressing concern, and being assertive, lead to changes in the way the doctor interacts with the patient.
References
-
- Bach PB, Cramer LD, Warren JL, Begg CB. Racial differences in the treatment of early-stage lung cancer. N Engl J Med. 1999;341:1198–205. - PubMed
-
- Petersen LA, Wright SM, Peterson ED, Daley J. Impact of race on cardiac care and outcomes in veterans with acute myocardial infarction. Med Care. 2002;40(suppl):I86–96. - PubMed
-
- Coronary heart disease mortality trends among whites and blacks—Appalachia and United States, 1980–1993. Morb Mortal Wkly Rep. 1998;47:1005–8. [No authors listed]. - PubMed
-
- Canto JG, Allison JJ, Kiefe CI, et al. Relation of race and sex to the use of reperfusion therapy in Medicare beneficiaries with acute myocardial infarction. N Engl J Med. 2000;342:1094–100. - PubMed
-
- Pratto F, Bargh JA. Stereotyping based on apparently individuating information: trait and global components of sex stereotypes under attention overload. J Exp Soc Psychol. 1991;l27:26–47.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical