

Implementing guidelines in primary care: can population impact measures help?
- PMID: 12542840
- PMCID: PMC149228
- DOI: 10.1186/1471-2458-3-7
Implementing guidelines in primary care: can population impact measures help?
Abstract
Background: Primary care organisations are faced with implementing a large number of guideline recommendations. We present methods by which the number of eligible patients requiring treatment, and the relative benefits to the whole population served by a general practice or Primary Care Trust, can be calculated to help prioritise between different guideline recommendations.
Methods: We have developed measures of population impact, "Number to be Treated in your Population (NTP)" and "Number of Events Prevented in your Population (NEPP)". Using literature-based estimates, we have applied these measures to guidelines for pharmacological methods of secondary prevention of myocardial infarction (MI) for a hypothetical general practice population of 10,000.
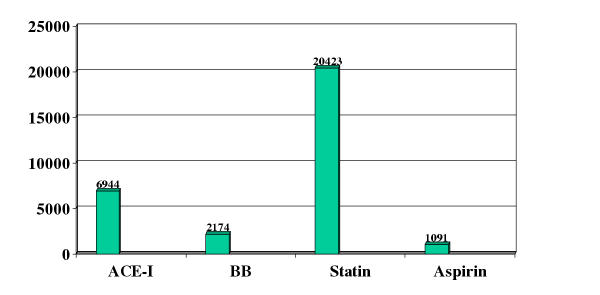
Results: Implementation of the NICE guidelines for the secondary prevention of MI will require 176 patients to be treated with aspirin, 147 patients with beta-blockers and with ACE-Inhibitors and 157 patients with statins (NTP). The benefit expressed as NEPP will range from 1.91 to 2.96 deaths prevented per year for aspirin and statins respectively. The drug cost per year varies from euro 1940 for aspirin to euro 60,525 for statins. Assuming incremental changes only (for those not already on treatment), aspirin post MI will be added for 37 patients and produce 0.40 of a death prevented per year at a drug cost of euro 410 and statins will be added for 120 patients and prevent 2.26 deaths per year at a drug cost of euro 46,150. An appropriate policy might be to reserve the use of statins until eligible patients have been established on aspirin, ACE-Inhibitors and beta blockers.
Conclusions: The use of population impact measures could help the Primary Care Organisation to prioritise resource allocation, although the results will vary according to local conditions which should be taken into account before the measures are used in practice.
Figures
Similar articles
-
[Secondary prevention after cardiac infarct; therapeutic efficiency--cost-benefit ratio].Internist (Berl). 2001 May;42(5):713-9. doi: 10.1007/s001080050812. Internist (Berl). 2001. PMID: 11400578 Review. German. No abstract available.
-
Cost-effectiveness of optimal use of acute myocardial infarction treatments and impact on coronary heart disease mortality in China.Circ Cardiovasc Qual Outcomes. 2014 Jan;7(1):78-85. doi: 10.1161/CIRCOUTCOMES.113.000674. Epub 2014 Jan 14. Circ Cardiovasc Qual Outcomes. 2014. PMID: 24425706 Free PMC article.
-
Rationale and design of the Post-MI FREEE trial: a randomized evaluation of first-dollar drug coverage for post-myocardial infarction secondary preventive therapies.Am Heart J. 2008 Jul;156(1):31-6. doi: 10.1016/j.ahj.2008.03.021. Epub 2008 Jun 6. Am Heart J. 2008. PMID: 18585494 Free PMC article. Clinical Trial.
-
Should patients receive secondary prevention medications for free after a myocardial infarction? An economic analysis.Health Aff (Millwood). 2007 Jan-Feb;26(1):186-94. doi: 10.1377/hlthaff.26.1.186. Health Aff (Millwood). 2007. PMID: 17211028
-
[Pharmacological prevention of coronary relapses in Italian clinical practice: a literature review].G Ital Cardiol (Rome). 2012 Nov;13(11):734-40. doi: 10.1714/1168.12949. G Ital Cardiol (Rome). 2012. PMID: 23096582 Review. Italian.
Cited by
-
Population impact of stricter adherence to recommendations for pharmacological and lifestyle interventions over one year in patients with coronary heart disease.J Epidemiol Community Health. 2005 Dec;59(12):1041-6. doi: 10.1136/jech.2005.035717. J Epidemiol Community Health. 2005. PMID: 16286491 Free PMC article.
-
Will changes in primary care improve health outcomes? Modelling the impact of financial incentives introduced to improve quality of care in the UK.Qual Saf Health Care. 2004 Jun;13(3):191-7. doi: 10.1136/qhc.13.3.191. Qual Saf Health Care. 2004. PMID: 15175489 Free PMC article.
-
Prioritising between direct observation of therapy and case-finding interventions for tuberculosis: use of population impact measures.BMC Med. 2006 Dec 20;4:35. doi: 10.1186/1741-7015-4-35. BMC Med. 2006. PMID: 17181867 Free PMC article.
-
Potential population impact of the UK government strategy for reducing the burden of coronary heart disease in England: comparing primary and secondary prevention strategies.Qual Saf Health Care. 2006 Oct;15(5):339-43. doi: 10.1136/qshc.2005.017061. Qual Saf Health Care. 2006. PMID: 17074870 Free PMC article.
-
Helping to prioritise interventions for depression and schizophrenia: use of Population Impact Measures.Clin Pract Epidemiol Ment Health. 2006 Mar 22;2:3. doi: 10.1186/1745-0179-2-3. Clin Pract Epidemiol Ment Health. 2006. PMID: 16553956 Free PMC article.
References
-
- NICE guideline on prophylaxis for patients who have experienced a myocardial infarction (html version). http://www.nice.org.uk/Docref.asp?d=16479
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
