

The lack of effect of market structure on hospice use
- PMID: 12546285
- PMCID: PMC1464044
- DOI: 10.1111/1475-6773.10562
The lack of effect of market structure on hospice use
Abstract
Objective: To describe the relative importance of health care market structure and county-level demographics in determining rates of hospice use.
Data sources: Medicare claims data for a cohort of elderly patients newly diagnosed with lung cancer, colon cancer, stroke, or heart attack in 1993, followed for up to five years, and linked to Census and Area Resource File data.
Study design: Variation between markets in rates of hospice use by patients with serious illness was examined after taking into account differences in individual-level data using hierarchical linear models. The relative explanatory power of market-level structure and local demographic variables was compared.
Data collection methods: The cohort was defined within the Medicare hospital claims data using validated algorithms to detect incident cases of disease with a three-year lookback. Use of hospice was determined by linkage at an individual level to the Standard Analytic Files for Hospice through 1997. Individual-level data was linked to the Area Resource File using county identifiers present in the Medicare claims.
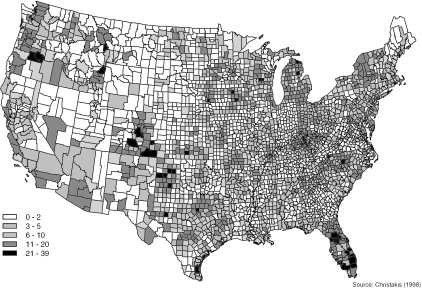
Principal findings: There is substantial variation in hospice use across markets. This variation is not explained by differences in the major components of health care infrastructure: the availability of hospital, nursing home, or skilled nursing facilities, nor by the availability of HMOs, doctors, or generalists.
Conclusions: Intercounty heterogeneity in hospice use is substantial, and may not be related to the set-up of the medical care system. The important local factors may be local preferences, differences in the particular mix of services provided by local hospices, or differences in community leadership on end of life-issues; many of these differences may be amenable to educational efforts.
Figures
References
-
- Allison PD. Survival Analysis Using the SAS System: A Practical Guide. Cary, NC: SAS Institute; 1995.
-
- Benesch C, Witter DM, Jr, Wilder AL, Duncan PW, Samsa GP, Matchar DB. “Inaccuracy of the International Classification of Disease (ICD-9-CM) in Identifying the Diagnosis of Ischemic Cerebrovascular Disease.”. Neurology. 1997;49:660–4. - PubMed
-
- Bryk AS, Raudenbush SW. Hierarchical Linear Models. Newbury Park, CA: Sage; 1992.
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. “A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation.”. Journal of Chronic Disease. 1987;40:373–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
