

HLA-DR2 dose effect on susceptibility to multiple sclerosis and influence on disease course
- PMID: 12557126
- PMCID: PMC1180245
- DOI: 10.1086/367781
HLA-DR2 dose effect on susceptibility to multiple sclerosis and influence on disease course
Abstract
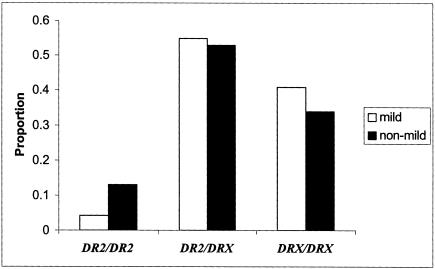
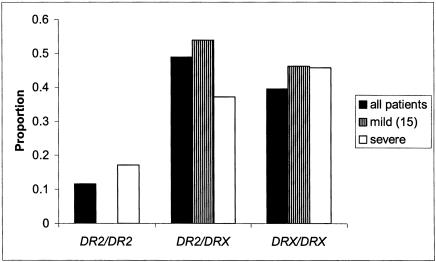
Models of disease susceptibility in multiple sclerosis (MS) often assume a dominant action for the HLA-DRB1*1501 allele and its associated haplotype (DRB1*1501-DQB1*0602 or DR2). A robust and phenotypically well-characterized MS data set was used to explore this model in more detail. A dose effect of HLA-DR2 haplotypes on MS susceptibility was revealed. This observation suggests that, in addition to the role of HLA-DR2 in MS, two copies of a susceptibility haplotype further increase disease risk. Second, we report that DR2 haplotypes modify disease expression. There is a paucity of benign MS and an increase of severe MS in individuals homozygous for DR2. Concepts of the molecular mechanisms that underlie linkage and association of the human leukocyte antigen (HLA) region to MS need to be revised to accommodate these data.
Figures

References
Electronic-Database Information
-
- Duke University Center for Human Genetics, http://wwwchg.mc.duke.edu/software/pdt.html (for Pedigree Disequilibrium Test computer program; a beta version of the geno-PDT program for genotype analysis is also available upon request: emartin@chg.mc.duke.edu)
-
- Online Mendelian Inheritance in Man (OMIM), http://www.ncbi.nlm.nih.gov/Omim/ (for MS [MIM 126200], DRB1 [MIM 142857], and DQB1 [MIM 604305])
References
-
- Allegretta M, Nicklas JA, Sriram S, Albertini RJ (1990) T cells responsive to myelin basic protein in patients with multiple sclerosis. Science 247:718–721 - PubMed
-
- Barcellos LF, Oksenberg JR, Green AJ, Bucher P, Rimmler JB, Schmidt S, Garcia ME, Lincoln RR, Pericak-Vance MA, Haines JL, Hauser SL (2002) Genetic basis for clinical expression in multiple sclerosis. Brain 125:150–158 - PubMed
-
- Barcellos LF, Schito AM, Rimmler JB, Vittinghoff E, Shih A, Lincoln R, Callier S, Elkins MK, Goodkin DE, Haines JL, Pericak-Vance MA, Hauser SL, Oksenberg JR (2000) CC-chemokine receptor 5 polymorphism and age of onset in familial multiple sclerosis. Multiple Sclerosis Genetics Group. Immunogenetics 51:281–288 - PubMed
-
- Beck J, Rondot P, Catinot L, Falcoff E, Kirchner H, Wietzerbin J (1988) Increased production of interferon gamma and tumor necrosis factor precedes clinical manifestation in multiple sclerosis: do cytokines trigger off exacerbations? Acta Neurol Scand 78:318–323 - PubMed
-
- Bertrams J, Kuwert E (1972) HL-A antigen frequencies in multiple sclerosis: significant increase of HL-A3, HL-A10 and W5, and decrease of HL-A12. Eur Neurol 7:74–78 - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
