

Accurate molecular detection of melanoma nodal metastases: an assessment of multimarker assay specificity, sensitivity, and detection rate
- PMID: 12560463
- PMCID: PMC1187289
- DOI: 10.1136/mp.56.1.43
Accurate molecular detection of melanoma nodal metastases: an assessment of multimarker assay specificity, sensitivity, and detection rate
Abstract
Background: The application of lymphoscintigraphy followed by sentinel lymph node (SN) biopsy to patients with primary melanoma has revolutionised the ability to identify accurately, yet conservatively, those patients who harbour occult nodal metastases. The molecular detection of SN micrometastases facilitates the cost effective analysis of the entire SN using multiple markers. Currently, a lack of marker specificity is the main barrier preventing the molecular evaluation of SN tissue from becoming clinically applicable.
Aims: To develop a reproducible multimarker reverse transcription-polymerase chain reaction (RT-PCR) assay, with the emphasis on achieving high specificity for the accurate detection of melanoma metastases in nodal tissue.
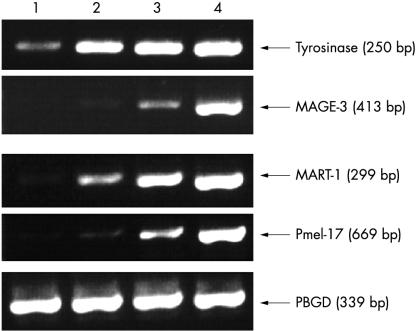
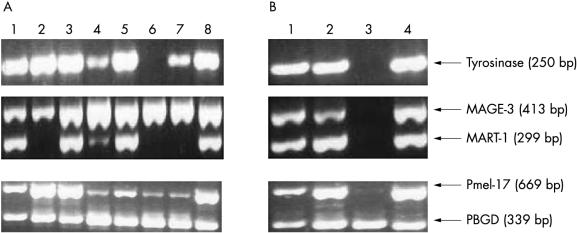
Methods: Three pigment cell specific (PCS) markers-tyrosinase, Pmel-17, and MART-1-and one cancer testis antigen (CTA)-MAGE-3-were selected for use in a multimarker RT-PCR assay. The conditions for this assay were optimised.
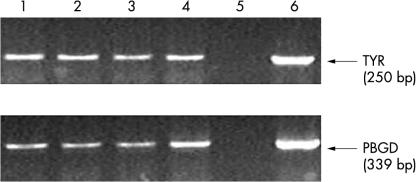
Results: High specificity was achievable for each marker by optimising the PCR cycle number such that unwanted transcripts (that is, illegitimate transcripts and/or specific transcripts from other low abundance nodal cell types) remained undetectable in appropriate controls (normal visceral nodes). Tyrosinase was 100% specific at 40 PCR cycles, MAGE-3 and MART-1 at 35 PCR cycles, and Pmel-17 at 30 PCR cycles. Tyrosinase proved to be the most sensitive marker, detecting 10 melanoma cells in 0.1 g of nodal tissue.
Conclusions: Excellent reproducibility of the entire nodal processing and RT-PCR protocol for the detection of very low numbers of melanoma cells in nodal tissue was shown, although there is a risk of false positives using the PCS markers alone, because of an approximate 4-8.5% incidence rate of nodal nevi in melanoma draining SNs (these nevi being absent in all other normal nodes). MAGE-3 was shown to be the only marker that is not expressed by melanocytes. However, because not all melanomas express MAGE-3, it is recommended that more emphasis should be placed on the development of a panel of CTA markers to ensure a zero false positive rate and to provide optimum detection.
Figures


References
-
- Reeves ME, Coit DG. Melanoma. A multidisciplinary approach for the general surgeon. Surg Clin North Am 2000;80:581–601. - PubMed
-
- Halpern AC, Schuchter LM. Prognostic models in melanoma. Semin Oncol 1997;24:S2–7. - PubMed
-
- Balch CM, Milton GW, Cascinelli N, et al. Elective lymph node dissection: pros and cons. In: Balch CM, Houghton AN, Milton GW, et al, eds. Cutaneous melanoma. Philadelphia: Lippincott, 1992:345–66.
-
- Shivers SC, Wang X, Li W, et al. Molecular staging of malignant melanoma: correlation with clinical outcome. JAMA 1998;280:1410–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical